Download
1 / 17
190 likes | 590 Views
Peripartum Cardiomyopathy. Paul M. Johnson Department of Internal Medicine University of North Carolina Hospitals November 11, 2009. Overview. Defining PPCM Incidence Etiology Diagnosis Treatment Prognosis Our patient today… Key Points.

E N D
Peripartum Cardiomyopathy Paul M. Johnson Department of Internal Medicine University of North Carolina Hospitals November 11, 2009
Overview • Defining PPCM • Incidence • Etiology • Diagnosis • Treatment • Prognosis • Our patient today… • Key Points http://www.e-heart.org/Pages/03_Cardiomyopathy/03_Cardiomyopathy_DCM_001.htm
How to define PPCM • NHLBI Workshop on Peripartum Cardiomyopathy (2000) • development of heart failure in the last month of pregnancy or five months after delivery • no pre-existing heart disease • no determinable cause of cardiomyopathy • LV systolic dysfunction defined by LVEF <45% or reduced shortening fraction (30% on M-mode) JAMA 2000; 283: 1183-8
Incidence “These Hausa-Fulani womeneat large quantities of a local lake salt, kanwa, for 40 days postpartum.The syndrome is markedly more common in the hot rainy season, whenevaporative water loss is less, than in the dry season. The firstpostpartum days are spent confined to bed in a small heated room. Once ortwice daily the new mother is given hot baths with branches which have beendipped in boiling water. The combination of excessive sodium intake anddiminished evaporative water excretion seems to precipitate failure in bothnormotensive and hypertensive patients.” -Circulation. 1977; 56: 1058-1061
Incidence of PPCM • Reported incidence is highly variable • Nigeria • among the Hausa in Zaria, as high as 1 per 100 live births • up to 13% of hospital admissions for females • Haiti • 1 per 300 live births • South Africa • 1 per 1000 • United States • between 1 per 3000 to 1 per 4000 live births • about 1300 women per year, mortality of up to 5% • a reported geographic predilection for Southern states Int J Cardiol 2007; 118: 295-303
Risk factors for PPCM • advanced age >30 • multiparity • African descent • multiple gestation • obesity • preeclampsia/eclampsia • hypertension • prolonged (>4 weeks) tocolysis with beta agonists • risk factors remain poorly understood Int J Cardiol 2007; 118: 295-303
What causes PPCM? Lancet 2006; 368: 687–93
Etiology, in other words • most cases are idiopathic • myocarditis • predisposition to more severe forms of viral myocarditis (8.8% - 76% prevalence) • autoimmune • fetal antigen response • chimerism • hemodynamic • inc blood volume • inc cardiac output Lancet 2006; 368: 687–93
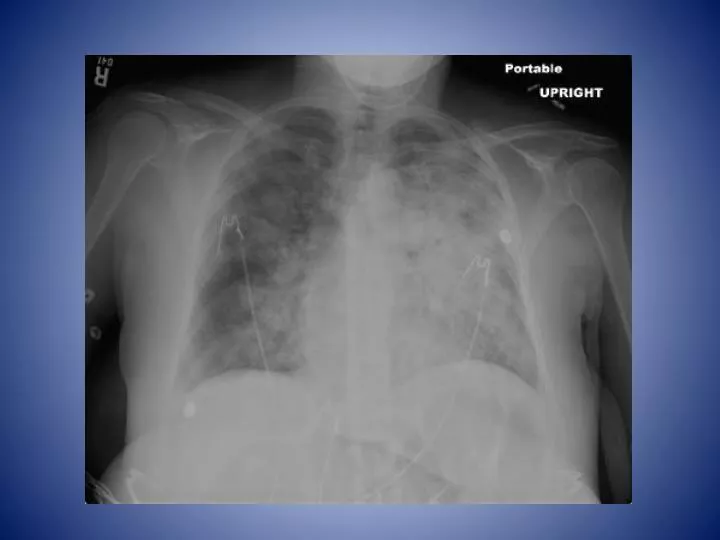
Diagnosis • DOE, fatigue, pedal edema can be normal in pregnancy • Be aware of warning signs • PND, crackles, JVD • CXR • cardiomegaly, edema, pleural effusions • EKG • normally NSR, but occasionally LVF, TWIs, Q wave • Must have ECHO for diagnosis
Treatment of PPCM • Similar to other types of CHF • optimize hemodynamics • relief of symptoms • chronic therapies that improve long-term outcomes • Specifically • avoid ACEI in pregnancy (OK in breast feeding) • use of hydralazine, digoxin acceptable • Anticoagulation • consider in LVEF <30% • Transplant • 4-7% of patients • successful pregnancies after transplant • Immunosuppression in myocarditis-mixed results, never empirically
Prognosis • prognosis related to related to LV recovery • 50% recover baseline function within 6 months www.uptodate.com from Felker et. al. N Engl J Med 2000; 342: 1077
Prognosis-another pregnancy? • Recovered LV function • 28 women • LVEF decreased 20% in 6 women • 6 women got HF • no deaths • Persistent LV dysfunction • 16 women • three deaths • HF in 7 patients • premature delivery in 6, therapeutic abortion in four Lancet 2006; 368: 687–93 NEJM 2001; 344: 1567
Our patient today… • admitted to cardiology with sore throat and TWI on EKG five days ago • diagnosed with strep throat and discharged with amoxicillin x 10 days • ECHO showed EF 50-55%
Key Points • PPCM diagnosed in 1 per 3000 to 4000 births/year • Etiology is likely multifactorial, and still unclear • Set diagnostic criteria • no previous disease, no other cause • onset one month before, five months after birth • LVEF < 45% • 50% regain normal LVEF, 50% do not • No guidelines for subsequent pregnancies
References • Abboud, J, et. al. Peripartum cardiomyopathy: A comprehensive review. Int J of Cardiol2007; 118: 295-303. • Bales, AC, and Lang, RM. Peripartum cardiomyopathy. Accessed 11/10/09 at www.uptodate.com • Elkayam, U, et. al. Maternal and fetal outcomes of subsequent pregnancies in women with peripartum cardiomyopathy. NEJM 2001; 344: 1567 • Fillmore, SJ, and Perry, EH. The evolution of peripartal heart failure in Zaria, Nigeria. Some etiologic factors. Circulation. 1977;56:1058-1061 • Rhamaraj, R, and Sorrell, VL. Peripartum cardiomyopathy: causes, diagnosis, and treatment. ClevClin J Med. 2009; 76: 289-296 • Sliwa, K, et. al. Peripartum cardiomyopathy. Lancet. 2006 Aug 19;368(9536):687-93.