Download
1 / 47
470 likes | 618 Views
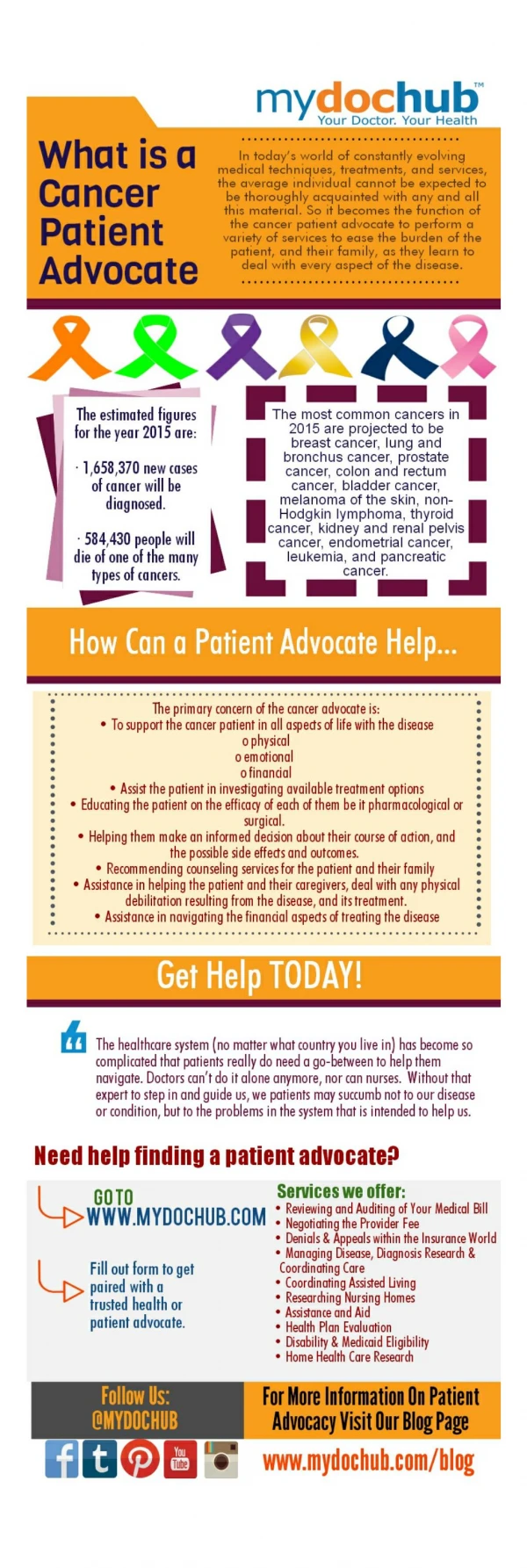
CONSUMER ACCESS TO PUBLIC REPORTING ON P4P RESULTS. 2005 HMO Report Card Office of the Patient Advocate Ed Mendoza Acting Director John Zweifler, MD, MPH Medical Consultant National Pay for Performance Summit. MISSION Office of the Patient Advocate. To inform and educate consumers

E N D
CONSUMER ACCESS TO PUBLIC REPORTING ON P4P RESULTS 2005 HMO Report Card Office of the Patient Advocate Ed Mendoza Acting Director John Zweifler, MD, MPH Medical Consultant National Pay for Performance Summit
MISSIONOffice of the Patient Advocate • To inform and educate consumers • about their rights and responsibilities • as HMO enrollees.
STATUTORY MANDATESOffice of the Patient Advocate • HMO Quality Report Card • Consumer Education • Advice and Assistance to HMO Enrollees • Recommendations to DMHC • Collaboration with Other Organizations
OBJECTIVESHMO Report Card • To provide comparative quality information for consumers, purchasers, regulators, and advocates. • To “incentivize” quality improvement through public disclosure. • To educate consumers about health care quality.
BASIC FEATURESHMO Report Card • Scope & Data Sources • Methodology • Presentation • Outreach and Distribution
California’s 10 largest HMOs -- 95% of all commercial enrollees (HEDIS & CAHPS) 200+ medical groups – 85% of all commercial and Medicare enrollees (HEDIS & CAS) Language services information for 10 commercial and 18 Medi-Cal plans (OPA Survey) SCOPE & DATA SOURCESHMO Report Card
HEALTH PLAN METHODOLOGYHMO Report Card Four Summary Star “Grades” (30 individual clinical & patient satisfaction scores): • Staying Healthy (10 scores) • Getting Better (9 scores) • Living with Illness (10 scores) • Member Rating of Health Plan (1 score)
MEDICAL GROUP METHODOLOGYHMO Report Card Six Summary Star “Grades” (29 individual scores): • Getting the Right Medical Care (9 scores) • Patient Rating of Care (20 scores) - Coordinating Patient Care (3 scores) - Timely Care & Service (9 scores) - Getting Treatment & Specialty Care (4 scores) - Communicating with Patients (4 scores)
LANGUAGE SERVICES DATAHMO Report Card Does the health plan provide: • Telephone interpretation services? • Access to face-to-face interpreters? • Bilingual provider lists? • Non-English written materials?
PRESENTATIONHMO Report Card • Web-Based • Comparative • Interactive • Printed Summary • English, Spanish, Chinese
MEDICAL GROUP RATINGS SUMMARYSacramento County - 2005 HMO Report Card
MEDICAL GROUP RATINGS SUMMARY West Los Angeles, 2005 HMO Report Card
MEDICAL GROUP RATINGS SUMMARY Sacramento County, 2005 HMO Report Card
MED GP DRILL DOWN – HEDIS SCORESSacramento County, 2005 HMO Report Card
MED GP DRILL DOWN – CHLAMYDIASacramento County, 2005 HMO Report Card
MEDICAL GROUP RATINGS SUMMARY Sacramento County, 2005 HMO Report Card
MED GP DRILL DOWN – CAS SCORESSacramento County, 2005 HMO Report Card
MED GP DRILL DOWN – TIMELY CARESacramento County, 2005 HMO Report Card
MED GP DRILL DOWN – VISITS ON TIMESacramento County, 2005 HMO Report Card
MED GP DRILL DOWN – DR EXPLAINSSacramento County, 2005 HMO Report Card
DISTRIBUTION OF PRINTED SUMMARIES2005 HMO Report Card • Local Pharmacies (574) • Public Libraries (500+) • Community-Based Organizations (500+ Events) • Website Downloading/Printing • Order Copies Toll-Free @ 1-866-HMO-8900
EVALUATION CRITERIAHMO Report Card • Use • Usability • Usefulness
ANNUAL USE DATA – PRINTED SUMMARYHMO Report Card * Partial year data for Year 5
EVALUATION DATA SOURCESHMO Report Card • Academic Research • User Focus Groups, Online Survey • Industry & Consumer Advocates • Report Card Partners • Formal Evaluation
LESSONS LEARNED – USERSHMO Report Card • Consumers: • are not aware of quality differences • are more interested in plan service than quality • prefer the detailed website to the printed summary • prefer Health Topics to the 4 summary categories • want to be able to customize the data even more • want more plan data on the website (e.g., cost) • prefer data reporting from an “objective” 3rd party
LESSONS LEARNED – INDUSTRYHMO Report Card • Health Plans and Medical Groups: • are very familiar with the Report Card • use the data to “benchmark” their performance and expect to improve over time • use the data for marketing and rate negotiations • believe the summary grades do not accurately reflect their performance • want separate/additional reporting for Medi-Cal • support the continuation of the Report Card
NEW SOURCES OF DATAHMO Report Card • OSHPD Hospital Discharge Data • Population-Based Surveys - California Health Interview Survey - Behavioral Risk Factor Surveillance Survey • OPA Surveys -
NEW USES OF DATAHMO Report Card • Efficiency Measures (HEDIS) • Health Disparities (HEDIS, CAHPS, CAS) • Preventable Hospitalizations (OSHPD, CHIS) • Disability Access Services (OPA) -
Sponsored by CDC and states Telephone survey of 2,000-6,000 adults/state Core questions; states can customize Targets alcohol and drug use, health status, prevention, utilization, and access Collects gender, age, education, race/ethnicity, household income, employment status, marital status, AND health plan membership SCOPE OF DATABehavioral Risk Factor Surveillance System
Have a Personal Doctor: White 71%, African American 64%, Hispanic 65% Did Not Get Needed Care: White 18%, African American 27%, Hispanic 23% Note: Little racial/ethnic variability for some measures – getting appointments as soon as wanted; physical and mental composite summary scores HEALTH RISK & STATUS FINDINGSBRFSS 2004 (Oregon)
Biennial, population-based, telephone survey (sample: ~50,000 households) Demographic, health status, utilization, AND health plan membership data Ethnic/language sub-populations over-sampled to provide additional stratification capacity SCOPE OF DATA California Health Interview Survey (UCLA)
16% of Californians, and 20% of Latinos and African Americans reported needing mental health services 42% of Californians reporting needing mental health received mental health services Minorities 30% less likely to receive mental health services LEP 80% less likely to receive mental health services after controlling other variables Lack of insurance reduced services by 50% Sentell P.California Program on Access to Care Findings. February 10, 2005 MENTAL HEALTH FINDINGSCHIS 2001
Racial and Ethnic Disparities in Healthcare in California (November, 2003) Blacks w/ higher admit rates than whites for CHF, asthma, diabetes, and hypertension Hispanics w/ higher admit rates for perforated appendix, lower for pneumonia and dehydration SOURCE OF DATA OSHPD Hospital Discharge Data
Angiography: Whites 23.4%, Blacks 20.6%, Hispanics 24.6% Percutaneous Coronary Intervention: Whites 22.9%, Blacks 13.4%, Hispanics 17.7% CABG: Whites 5.0%, Blacks 2.7%, Hispanics 4.4% 30 day mortality for MI: Whites 13.04%, Blacks 12.50%, Hispanics 12.91% DISPARITIES – ANGINA & MI ADMISSIONSCA OSHPD Data (1999-2001)
OTHER POTENTIAL EXPANSIONSHMO Report Card • Product Lines: - Medi-Cal - Healthy Families - Medicare • Provider Types: - Individual Physicians - Hospitals - Skilled Nursing Facilities
Transparency for Consumers Comprehensive Information Adjustment for Known Variables Acknowledgement of Data Limitations CONSIDERATIONSEquity and Public Reporting
ISSUES & CONSIDERATIONSHMO Report Card • Absolute vs. Relative Scoring • Consumer Use vs. Industry Use • Data Usability vs. Data Precision • Consumer Usefulness vs. Available Data • Voluntary vs. Mandatory Participation
ACKNOWLEDGMENTSHMO Report Card Project • California Cooperative Healthcare Reporting Initiative • Integrated Healthcare Association • Pacific Business Group on Health & Sapient Corporation • OPA Cultural & Linguistic Services Work Group • Walgreens, Leader, Independent Pharmacies • California Association of Health Plans • Local Health Plans of California • Participating Health Plans and Medical Groups
SAVE THE DATEOPA Symposium on Public Disclosure Challenges and Opportunities in Quality Reporting Statewide Policy Implications June 6, 2006 Crowne Plaza Hotel – LAX Los Angeles, California
WEB ADDRESSHMO Report Card VISIT hmoreportcard.ca.gov