Download
1 / 20
200 likes | 349 Views
PREMUS 2001, Amsterdam. A Case-Control Study of Biomechanical and Psychosocial Risk Factors for Occupational Low-Back Pain. Michael S. Kerr, PhD Institute for Work & Health Toronto, Ontario, CANADA. Kerr et al. (2001) Am J Pub Health 91:1069-1075. Study Collaborators.

E N D
PREMUS 2001, Amsterdam A Case-Control Study of Biomechanical and Psychosocial Risk Factors for Occupational Low-Back Pain Michael S. Kerr, PhD Institute for Work & Health Toronto, Ontario, CANADA Kerr et al. (2001) Am J Pub Health 91:1069-1075
Study Collaborators Institute for Work & Health: Kerr MS, Frank JW, Shannon HS, Bombardier C University of Waterloo: Norman RW, Wells RW, Neumann P General Motors: Mr. Elmer Beddome CAW: Mr. John Graham The Ontario Universities Back Pain Study (OUBPS) Group Andrews D, Beaton DE, Dobbyn M, Edmonstone E, Ferrier S, Hogg-Johnson S, Ingelman P, Mondlock M, Peloso P, Smith J, Stanfield SA, Tarasuk V, Woo H
Why a case-control study? • Uncertainty about role of physical demands necessitated concentration of effort on developing valid workplace measures • Cohort model required multiple measures at multiple times to assess valid exposure Does a prospective cohort study with limited (e.g. once only) exposure assessment really provide more rigorous evidence than a case-control study with more detailed assessments?
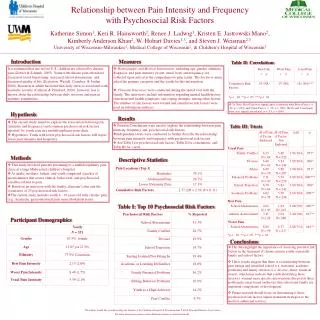
Research Question After controlling for individual characteristics, what are the main work-related biomechanical and psychosocial risk factors for reported low-back pain?
STUDY SETTING GM-Oshawa autoplex 65 km east of Toronto Total hourly-paid work force – approx. 12,000 3 Divisions: Car Assembly (7,000) Truck Assembly (3,000) Fabrications N/A Nursing stations – handle ALL WCB reports as well as most other health problems occurring at work-site Truck = 1 station; Car = 4 stations
The GM Study of Low-back Pain Incidence density sampling workers without LBP 10,000 car and truck plant workers (hourly-paid) STUDY POPULATION random selection (job-matched) (n=137) CASES accrued via workplace health stations workers with LBP CONTROLS (n=179) baseline conducted at home questionnaire and (n2=65) physical exam at work doing usual job video, EMG, checklists, posture physical demands assessment
SUBJECT ENROLMENT 179 A total of 381 subjects enrolled in the study Random controls (Voluntary) Cases 65 Job-matched controls (used for proxy data) 137
CASE Definition • Full-time, hourly-paid worker with “sprain-strain” LBP (reported to nursing stations) • No lost-time or WCB claim requirement • No previous worksite LBP report (90 days)
Were cases and controls comparable except for LBP? sd from male reference population SF-36, Health-related quality of life Physical Function Role – Physical Bodily Pain Social Function Vitality Role – Emotional Mental Health General Health Ref: Garrat et al. (1993) BMJ 306:1440-4
STUDY VARIABLES - 1 INDIVIDUAL Characteristics Age, height, weight, body mass index, sex education, marital status, preschool children, main wage earner, non-occupational physical activity, smoking, alcohol consumption
STUDY VARIABLES - 2 BIOMECHANICAL Factors (reduced a priori to about 20 key variables, NO EMG) • Peak Forces: • compression; shear; hand force • Cumulative Forces: • average and integrated compression; • Low-level (static) Forces: • compression • Posture and Movement: • peak flexion; time non-neutral; trunk kinematics
STUDY VARIABLES - 3 PSYCHOPHYSICAL Factors self-rated physical exertion measures distinct from "objective" measurements of physical demands analyses, but may also have additional role to play over and above the measured demands e.g. tolerance levels, "job stress", etc.
STUDY VARIABLES - 4 PSYCHOSOCIAL Factors • Karasek-Theorell Job Content Instrument • "psychological demand", decision latitude, supervisor support, coworker support, workplace social environment, job self-identity • - job dissatisfaction, mastery, empowerment, status inconsistency ("over-education")
Summary of Key Risk Factors (after adjusting for individual characteristics)
Study Strengths • Directly measured physical demands data combined with (basic) physical exam and interview-assisted psychosocial data for individual subjects • Comprehensive workplace job demands assessments (generalizable – i.e. not specific to automobile manufacturing) • Well defined study base for subject selection
Study Weaknesses • Modest participation rate (approx 60%) • Relied on workplace reporting mechanism to identify cases • Self-report only for psychosocial factors • Case-control design • But … does a prospective cohort study with limited once only exposure assessment really provide more rigorous evidence than a case-control study with more detailed assessments?
How did we control for Bias? • Directly measured physical demands data rather than self-report • Job-matched controls used to examine potential recall bias (none observed) • Used newly incident cases rather than prevalent cases • Compared cases with non-participating compensation claimants (no differences) • A priori reduction in variables eligible for regression modeling (multi-methods)
DIRECT EFFECTS INDIRECT EFFECTS e.g. job control BIOMECHANICAL LOAD PSYCHOSOCIAL LOAD TOLERANCE REDUCED TOLERANCE EXCEEDED TISSUE RESPONSE HORMONES e.g. cortisol MUSCLE TENSION e.g. cumulative compression BIOMECHANICAL LOAD PSYCHOSOCIAL LOAD Possible Biological Mechanisms
Main Conclusions • Consistency and strength indicates biomechanical load increases LBP risk • Psychosocial factors also shown to be associated with reporting LBP • Job dissatisfaction not a risk factor for reporting LBP in this setting • Psychosocial instruments (especially Karasek’s demands scale) may require further refinement for MSK studies
For additional information please contact: Mickey Kerr The Institute for Work & Health 481 University Ave., Suite 800 Toronto, ON M5G 2E9 Phone: (416) 927-2027 Fax: (416)-927-4167 Website: http://www.iwh.on.ca E-mail: info@iwh.on.ca The Institute for Work & Health operates with the support of the Ontario Workplace Safety & Insurance Board Kerr et al. (2001) Am J Pub Health 91:1069-1075