Download
1 / 12
160 likes | 395 Views
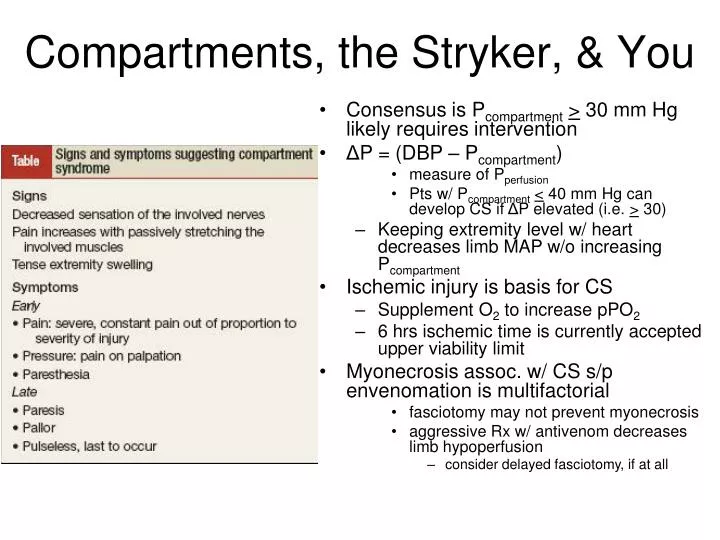
Consensus is P compartment > 30 mm Hg likely requires intervention Δ P = (DBP – P compartment ) measure of P perfusion Pts w/ P compartment < 40 mm Hg can develop CS if Δ P elevated (i.e. > 30) Keeping extremity level w/ heart decreases limb MAP w/o increasing P compartment

E N D
Consensus is Pcompartment> 30 mm Hg likely requires intervention • ΔP = (DBP – Pcompartment) • measure of Pperfusion • Pts w/ Pcompartment< 40 mm Hg can develop CS if ΔP elevated (i.e. > 30) • Keeping extremity level w/ heart decreases limb MAP w/o increasing Pcompartment • Ischemic injury is basis for CS • Supplement O2 to increase pPO2 • 6 hrs ischemic time is currently accepted upper viability limit • Myonecrosis assoc. w/ CS s/p envenomation is multifactorial • fasciotomy may not prevent myonecrosis • aggressive Rx w/ antivenom decreases limb hypoperfusion • consider delayed fasciotomy, if at all Compartments, the Stryker, & You
Possible Etiologies • Decreased volume • Hematoma • Trauma • crush injury & entrapment • compression during sleep/intoxication • Iatrogenic • prolonged lithotomy • MAST, casts, splints, dressings • excessive traction in line • tight closure of fascial defect • IV infiltration • Increased contents • Hematoma • Trauma • fracture • envenomation • burns • Increased use • exercise • tetany • seizure • eclampsia • Edema • nephrotic syndrome • ischemia-reperfusion injury • Iatrogenic • Orthopedic surgery • Intraarterial drug injection
Open sterile assembly • Place needle on tapered end of well chamber and syringe on opposite side • Place assembly into monitor, clear side of well chamber up
Purge assembly of air • Injecting NS w/ Stryker at 450 • Zero unit in position in which measurement will be taken • Sterile prep of site • Infiltrate local superficially • Enter compartment perpendicularly, level w/ heart • Inject ~ 0.3 of 1 cc saline • Read measurement on display when equilibrates • Re-Zero unit for each new measurement
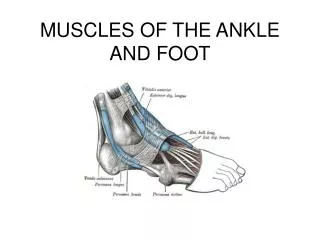
Enter compartments at junction of proximal & middle thirds of forearm Volar Compartment: btwn PL tendon & radial surface of ulna; depth 1-2 cm
Dorsal Compartment: 1-2 cm lat to posterior aspect of ulna; depth 1-2 cm Mobile Wad Compartment: lateral to radius; depth 1-1.5 cm
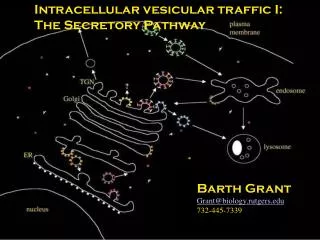
Enter compartments at junction of proximal & middle thirds of lower leg Lateral compartment: posterior border of fibula; depth 1-1.5 cm
Deep posterior compartment: posterior to medial border of tibia in direction of posterior border of the fibula; depth 2-4 cm Superficial posterior compartment: posteriorly directly over center of gastrocnemius; depth 1-1.5 cm
Anterior compartment: 1 cm lateral to anterior tibial border; depth 1-3 cm
Additional Compartments • Foot • Medial, Lateral, Interosseous • Gluteal • 18-G spinal needle • Depth 4-8 cm • Insert perpendicularly at point of max. tenderness
Improvised mercury or saline/sterile H2O manometers may also be zeroed & used to measure Pcompartment Convert mmHg cm H2O & back! References: JR Roberts and J Hedges, eds. Clinical Procedures in Emergency Medicine, 4th ed. Saunders; October 24, 2003. CB Custalow. Color Atlas of Emergency Department Procedures, 1st ed. Saunders; August 27, 2004.