Download

1 / 15
150 likes | 286 Views
DEFLATED LUNGS. High Frequency Percussive Ventilation HFPV. Subphysiologic tidal volumes Up to 900 breaths/ minute Pneumatically powered Time cycled Pressure limited Inspiratory and expiratory percussion. HFPV. Plateau. Plateau. Plateau. Baseline. Baseline. HFPV Class 1 Evidence.

E N D
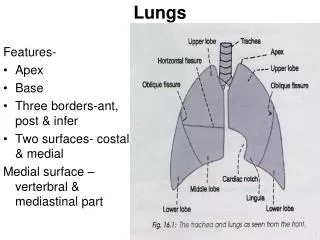
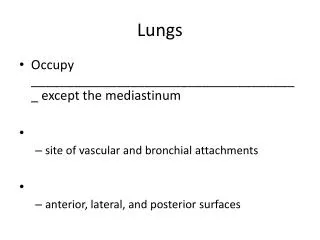
High Frequency Percussive VentilationHFPV • Subphysiologictidal volumes • Up to 900 breaths/minute • Pneumatically powered • Time cycled • Pressure limited • Inspiratory and expiratory percussion
HFPV Plateau Plateau Plateau Baseline Baseline
HFPV Class 1 Evidence • Improved oxygenation • FiO2 • PIP
18 Hours after HFPV • Improved pO2 • Decreased pulmonary edema
Returning to the case…. • Family consented • Procurement successful for heart, lung, liver and kidneys
Collaboration OPO and Intensivists
Summary • Recognition of Potential Organ Donor patients • Prompt ICU care focusing on lungs • Awareness of cofounding factors which impair oxygenation • Partnering with patient, family and OPO
Case study • 30 yo male, unhelmetedmotor cycle collision/ ejected injuries include: • TBI with multifocal intracranial hemorrhage/DAI. • Multiple facial and mandible fxs including multiple lacerations • Extensive craniofacial open wounds intubated closed head injury with ICH/ DAI/ cerebral edema • Pulmonary contusions/ aspiration • Declared post trauma day #3/ Organ donor with recovery post trauma day #6
Admission • Day 1: Bilateral contusions • VC/AC, TV 6/kg, PEEP 5, rate 18, I Time 0.9 sec • O2 - 80%, P/F ratio 250 • Day 3: Worsening atelectasis/ infiltrates/ contusions • Same vent settings, P 8 • ABG:7.28/48/80/-5/96% • P/F ratio 100 • Patient declared and is to be an organ donor
So what do you do now? • A) go to the OR and recover liver and kidneys because the lung function is too bad • B) increase the FiO2 to 100% • C) increase the rate to improve the respiratory acidosis • D) begin lung recruitment maneuvers • E) all of the above
Is the extra time for better lung management worth it? • Retrospective review: 400 consecutive donors of isolated lung recipients • Mechanism of donor BD-no effect • Management longer than 10 hrs results in better recipient survival (69% vs 58% at 5 years, 51% vs. 42% at 10 years, p <.05) • “Longer and better donor management” Wauters et al. Eur J Cardiothoracic surgery 2011; 39; e 68-e76.
Respiratory Goals in Donor Management • Optimize lung functionwhile minimizing ongoing injury to the lungs • Provide adequate oxygen delivery to support all organs in context of multi-organ recovery • Increase likelihood of lung recovery for lung transplantation
Historical Standard Lung Transplant Donor Criteria • Age < 55 • Clear Chest X-Ray • PaO2/FiO2 ratio >300mmHg on 100% FiO2,PEEP 5 • Absence of chest trauma • No evidence of aspiration, sepsis, purulent secretions at bronchoscopy • Sputum/BAL GS free of bacteria, fungus, significant white cells • Smoking History <20 pack years *these lungs don’t really exist