Download
1 / 17
190 likes | 342 Views
The Drug Development Process: Pharmaceutical Industry. Drug Development Altruistic Objective : Offer the public a therapeutic chemical compound to prevent or alleviate disease symptoms.

E N D
The Drug Development Process: Pharmaceutical Industry
Drug Development Altruistic Objective: Offer the public a therapeutic chemical compound to prevent or alleviate disease symptoms. Commercial Objective: Cost-effectively discover and develop a potentially therapeutic chemical compound that generates adequate revenues to… 1) Recover R&D costs of drug. 2) Sustain synthesis, distribution and marketing activities for drug. 3) Provide spending capital to fund new R&D activities.
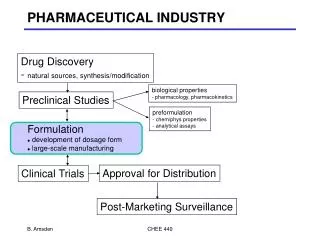
Categorical costs of drug discovery & development • Corporate infrastructure and overhead. • Intellectual protection and litigation. • Biological research. • Chemical research. • Preclinical safety assessment (toxicology). • FDA relations • Clinical safety assessment (phase 1 clinical trials). • Clinical efficacy assessment (phase 2 clinical trials). • Large scale synthesis and formulations. • Distribution. • Marketing & Sales Discovering and bringing one new drug to the public typically costs a pharmaceutical company nearly $1 billion and takes an average of 10 to 12 years.
“Brand name manufacturers” are given 17 years of patent life and allowance for restoration of up to 5 years of lost patent time due to delays in the drug approval process. Drug Development Timeline Cost Recovery Patent R&D Timeline Expiration of patent Date of patent application “Launch” date (drug is marketed to public)
Critical Stages of Drug Development (in chronological order) • Identification of drug “target” • Screening for chemical compounds that bind to “target” • Safety assessment (preclinical) • Safety assessment (clinical) • Efficacy assessment (clinical) • Clinical monitoring (post-launch) • Utilization of computational methods are expected to… • DECREASE TIME of development • INCREASE probability of drug approval
Identification of drug “target’ • A drug target is the receptor or enzyme that the drug will bind to and inactivate. • A) DNA microarray-based gene expression profiling in disease tissues to identify the genes (extrapolated to proteins) that show altered gene regulation in the disease state. • B) Identification of SNPs (or mutations) that confer the disease state.
2) Screening for chemical compounds that bind to “target” • A) 3D characterization and modeling of the target enzyme or protein for the purposes of identifying a region or domain of the protein that a drug can bind to (with high affinity). • B) Prediction of the molecular structure of a drug that will bind to the target. Use the principal components of this prediction to reduce the diversity (and number) of chemical compounds to be screened.
3) Safety assessment (preclinical) • DNA microarray focused on liver enzymes (metabolic enzymes) to characterize the response of the liver to the drug (in rats). • DNA microarray-based expression profiling in the target tissue to assess the response of the target tissue.
4) Safety assessment (clinical) • SNP screening in normal patients to correlate altered drug metabolism with known SNPs in drug metabolism enzymes. • Data from this represents the future of personalized medicine.
5) Efficacy assessment (clinical) A) Utilization of molecular endpoints in clinical studies (high-content assays)
6) Clinical monitoring (post-launch) • SNPs (known & new) identified in poor responders and toxicity issues. • SNP screening of metabolic enzymes (in the near future). • SNP screening of ALL known SNPs (in the next decade).
FDA Home Page | Search FDA Site | FDA A-Z Index | Contact FDA | FDA Centennial FDA Statement FOR IMMEDIATE RELEASEStatementDecember 3, 2006 Media Inquiries:Kristen Neese, 301-827-6242Consumer Inquiries:888-INFO-FDA Pfizer Stops All Torcetrapib Clinical Trials in Interest of Patient Safety On December 2, 2006, FDA was notified that Pfizer will suspend a large, Phase 3 trial evaluating the investigational cardiovascular therapy torceptrapib/atorvastatin (T/A) due to an increased rate of mortality (death) in patients receiving the combination compared to those receiving atorvastatin alone. With the T/A development program, as it does with all such development programs, FDA assured that Pfizer had the appropriate protections in place for patients participating in the drug’s development, including informed consent, a Data Safety Monitoring Board (DSMB) for its outcome study, and that the development program was done in a careful, stepwise manner. For this trial, the DSMB was conducting a monthly analysis of mortality data and a quarterly analysis of a number of outcomes including stroke, heart attack, and revascularizations (e.g., coronary stents or bypass surgery) to ensure the ongoing safety of patients in this trial. This independent board notified Pfizer of the mortality finding early the morning of December 2, 2006 and FDA was notified at 4:00 PM EST that evening that Pfizer planned to halt this trial and the development program overall. FDA fully supports Pfizer's decision to suspend this trial. The system of biomedical research monitoring was effective in this case, assuring that once a certain signal was seen, the trial was halted. FDA will continue to work with Pfizer and other sponsors developing molecules in this class of drugs to ensure that appropriate protections are in place to identify any safety signals as early in the development process as possible. Clinical trials are an integral part of the process for developing new medical innovations and the healthcare system is dependent upon this research, and the patients willing to participate, to advance therapies. Clinical trials often tell us unexpected things, both positive and negative, about new medical products, which is why carefully designed and conducted trials are an essential part of the pre-market process for demonstrating that new drugs are safe and effective before they can be approved for marketing.
Pfizer to cut 10,000 jobs, shut 5 plants No. 1 drugmaker unveils an additional $1 billion in restructuring moves; net income surges on sale of consumer health care business. By Aaron Smith, CNNMoney.com staff writer January 22 2007: 4:06 PM EST NEW YORK (CNNMoney.com) -- Pfizer announced Monday that it will cut 10,000 jobs and close five plants, including three R&D sites and two factories, by the end of 2008, and said its quarterly earnings grew but sales were little changed. In revealing an additional $1 billion in restructuring moves, Pfizer also said it does not expect sales to grow in 2007 and 2008, and that it might purchase up to $10 billion of its own stock. "There are no sacred cows" said Jeffrey Kindler, Pfizer's chief executive, at an analysts' meeting in New York to unveil the latest moves, which bring the company's total cost-saving effort to $5 billion. The world's biggest drug maker in terms of sales said the job cuts represent 10 percent of its worldwide work force. The cuts include the recently announced termination of 2,200 sales representatives in the U.S., meaning the number of new cuts is 7,800. The company said it plans to close three research sites in Michigan, including two facilities in Ann Arbor, and one in Kalamazoo. The company also plans to close manufacturing sites in Brooklyn, N.Y., and Omaha, Neb. The announcement was part of Pfizer's five-year plan to reduce its manufacturing plants from 93 to 48 by the end of 2008. Pfizer said it is also considering the closure of research sites in Japan and France, and it is also considering selling a factory in Germany, but all this is yet to be decided. The company plans to invest $3 billion of the money it saves in cost cuts in new products and business development through the end of 2008. "We fully understand that we cannot cost cut our way to long-term success," Kindler said. He said he hopes to triple the size of his late-stage pipeline by 2009, and for the company to generate four of its own new products per year beginning in 2011. The company's best hopes for growing sales took a blow in December, when studies of the experimental cholesterol drug torcetrapib were discontinued because of a high death rate and heart problems among patients. The decision to discontinue torcetrapib was "disappointing and brought into sharper focus the need to transform Pfizer over time to succeed in a dynamic healthcare marketplace," said Kindler in the statement. "We are reviewing every aspect of our business, and I look forward to discussing our priorities when we meet with analysts in New York." In addition to projecting flat sales growth for 2007 and 2008, Pfizer projected net income of $1.45 to $1.55 a share and operating income of $2.18 to $2.25 a share. For 2008, the company projected net income of $1.75 to $1.93 a share, and operating income of $2.31 to $2.45 a share. In 2007, Pfizer plans to expand its marketing of the inhalable insulin product Exubera. So far, Exubera has only been made available in very restricted quantities. But Ian Read, head of worldwide pharmaceutical operations, said there will be a "full-court press" roll-out of Exubera and direct-to-consumer advertising will begin in the second half of the year. Behind Pfizer, Johnson & Johnson is the second largest drugmaker in the U.S., followed by Abbott Laboratories (down $0.21 to $53.31, Charts), Merck (down $0.27 to $45.33, Charts), Bristol-Myers Squibb (down $0.12 to $26.51, Charts) and Wyeth (Charts).
Research Highlights Nature Reviews Drug Discovery 5, 722 (September 2006) | doi:10.1038/nrd2139 Cardiovascular disease: SNP to the rescue? Charlotte Harrison Can a common single nucleotide polymorphism (SNP) have sufficient impact to affect therapeutic targeting in heart disease? This possibility has recently been raised in a paper by Liggett and colleagues, who showed that a polymorphism in the 1-adrenergic receptor ( 1AR) altered cardiac function and response to the adrenergic receptor antagonist bucindolol in human heart failure. Clinical trials of 1AR antagonists in heart failure have often revealed substantial inter-individual variability in outcomes, which the authors considered could be due to differences in the 1AR gene. Indeed, the Liggett group had previously found a common non-synonymous SNP that results in either Arg or Gly being encoded at amino-acid position 389 of the 1AR. Compared with Gly- 1AR, Arg- 1AR displayed increased stimulation of adenylyl cyclase in transfected fibroblasts, enhanced contractility in transgenic mouse hearts and caused a larger increase in left ventricular ejection fraction after 1AR antagonist administration in human studies. The authors therefore set out to investigate the relevance of this SNP for 1AR antagonist therapy in heart failure by using bucindolol, a drug that has previously failed to show efficacy in clinical trials. Ventricular tissue from failing and non-failing human hearts was used to investigate the impact of 1AR genotype on contractile responses. In both heart types, Arg homozygotes displayed fourfold larger agonist-promoted contractility than Gly carriers. In transfected fibroblasts expressing 1ARs of either genotype, those expressing the Arg- 1AR displayed a substantially greater degree of noradrenaline-stimulated cAMP accumulation, and bucindolol showed a larger absolute cAMP-lowering effect in these cells compared with those expressing the Gly- 1AR. Continued Next Page…
To understand the clinical implications of the 1AR SNP, the authors undertook genotyping of the 1AR allele in patients who had taken part in a large placebo-controlled clinical trial of bucindolol for the treatment of moderate and severe heart failure. Each patient cohort consisted of >200 subjects, grouped by treatment and genotype. No outcome was associated with genotype in the placebo group, indicating little impact on the natural course of heart failure. However, Arg homozygotes treated with bucindolol had an age-, sex- and race-adjusted 38% reduction in mortality and 34% reduction in mortality or hospitalization compared with placebo. In contrast, Gly carriers had no change in clinical response to bucindolol compared with placebo. The therapeutic advantage of Arg homozygotes was due to the degree of adrenergic activity that could be antagonized by bucindolol. Although it has yet to be shown whether these results can be extrapolated to other 1AR antagonists with differing pharmacological properties to bucindolol, this study has shown that a drug that was not efficacious in a mixed patient population displayed greater efficacy in patients of a specific genotype, and so could set the stage for genetic-based treatments in heart failure.