Download
1 / 46
460 likes | 645 Views
Abdomen. N1037. Assessment of the Abdomen. Provides information regarding the functions of : gastrointestinal tract cardiovascular system genitourinary system. Anatomy and Physiology. Abdominal cavity - btwn the diaphram & symphysis pubis. Anatomy and Physiology. Peritoneum

E N D
Abdomen N1037
Assessment of the Abdomen • Provides information regarding the functions of : • gastrointestinal tract • cardiovascular system • genitourinary system
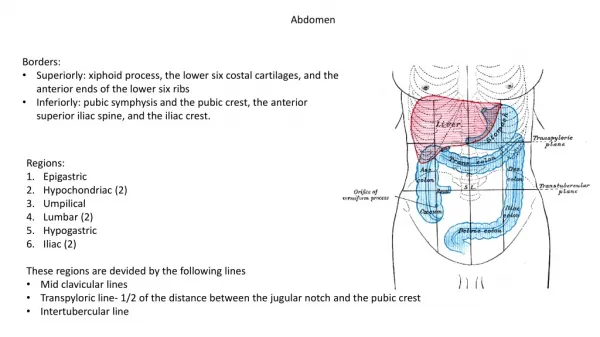
Anatomy and Physiology • Abdominal cavity - btwn the diaphram & symphysis pubis
Anatomy and Physiology • Peritoneum • 2 linings : parietal/viseral • intraperitoneum • spleen, gallbladder, liver, bile duct, stomach, sm & lrg intestine • retroperitoneum • pancreas, kidneys, ureters. bladder • linea alba - tendonous tissue • 4 muscles groups • abdominis rectus • transverse abdominis • external oblique • internal oblique
Anatomy and Physiology • Abdominal vasculature • descending aorta • abdominal aorta • L4 - aorta bifurcates into • R & L common iliac arteries • above umbilicus
Anatomical MappingAssessment Landmarks • 1. Xiphoid process • 2. Costal margin • 3. Abdominal midline • 4. Umbilicus • 5. Rectus abdominis muscle • 6. Ant superior iliac crest • 7. Inguinal ligament • 8. Symphysis pubis
Anatomy and Physiology • Stomach • J shaped, located in LUQ, under diaphram, R of spleen • reservoir for digestine (HCL acid + digestive enz) • liquefies foodstuff into chyme duodeum for dig + absorption • capacity = 1-1.5L , • Small intestine • 30 ft convoluted loops • extends form pyloric sphincter to ileocecal valve at lrg intestine • 3 segments • duodenum - digestion via common bile & pancreatic ducts • jejunum - nutrient absorption occurs • ileum - absorbs bile salts & Vit B12
Anatomy and Physiology • Large intestine • extends from ileocecal valve to anus • 4 segments (ascending, transverse, descending, colon) • forms stool & absorption of H20 & electrolytes • Liver • RUQ • storage, detoxification & filtraton, metabolism, synthesis & secretion • Gallbladder • pear shaped sac under liver • store & concentrate bile produced in liver • contracts , releases bile into cystic ducts to common bile duct into duodeneum
Anatomy and Physiology • Pancreas • URQ & ULQ of posterior abdominal wall • exocrine gland= secrets Bicarbonate &pancreatic enz for digestion • endocrine gland= secretes hormones (insulin, glucagon, gastrin) • Spleen • lymph organ in ULQ • filters (old and deformed RBC/platelets) • stores RBC for use in hemorrhage/exercise • Vermiform appendix • RLQ, fingerlike appendage • often obstructs with content from cecum
Anatomy and Physiology • Kidneys, ureters, and bladder • kidneys = bean shaped, at T12 & T13 posteriorly • Kidneys= rid body of waste products, maintain homeostasis via acid base balance, fluid & electrolyte balance, arterial BP • urine leaves kidneys via ureters to bladder =peristaltic wave • Bladder = stores urine (200-400ml) • Lymph nodes • inguinal area = deep & superficial lymph nodes • only superficial are palpable • inguinal & popliteal nodes
Health History • Patient profile • Age • Child to young adult: appendicitis • Adult: peptic ulcers, cholecystitis, diabetes mellitus • Gender • Female: gallbladder disease • Male: GI cancers, cirrhosis, duodenal ulcers
Common Chief Complaints • Nausea and vomiting • Diarrhea or constipation • Abdominal distension • Abdominal pain • Increased eructation or flatulence • Dysuria • Nocturia • Incontinence
Characteristics of Chief Complaint • Quality • Quantity • Associated manifestations • Aggravating factors • Alleviating factors • Setting • Timing
Past Health History • Medical • Abdomen specific • Nonabdomen specific • Surgical • GI procedures
Common Medications • Histamine-2 antagonists • PPI • Antibiotics • Lactulose • Antacids • Antidiarrheals • Laxatives or stool softeners • Antiemetics • Antiflatulents
Past Health History • Communicable diseases • Allergies • Injuries and accidents
Family Health History • Malignancies of stomach, liver, pancreas, colon; peptic ulcer disease, diabetes mellitus, irritable bowel syndrome, colitis
Social History • Alcohol use • Drug use • Travel history • Home and work environments • Hobbies and leisure activities • Economic status
Health Maintenance Activities • Sleep • Diet • Exercise • Stress management • Use of safety devices • Health check-ups
Assessment of the Abdomen • Equipment • Order ……NOTE CHANGE • Inspection • ***Auscultation*** • Percussion • Palpation
Inspection of Abdomen • Observe for : • Contour • Symmetry • Rectus abdominis muscles • Pigmentation and color • Scars • Striae • Respiratory movement • Masses or nodules • Visible peristalsis • Pulsation • Umbilicus
Inspection of Abdomen Normal Findings • Abdomen is flat or round, symmetrical • Uniform in color and pigmentation • No scars or striae present • No respiratory retractions • No masses or nodules • Ripples of peristalsis may be visible • Nonexaggerated pulsation of the abdominal aorta may be present • Umbilicus is depressed
Auscultation of Abdomen • Bowel sounds • Assess all four quadrants • Listen for at least 5 minutes before concluding bowel sounds are absent N = BS are heard in all quadrants • Usually are high pitched • Occur 5 to 30 times per minute Abnormal findings: • Absent or hypoactive BS indicate motility and possible obstruction • Hyperactive BS indicate motility and possible diarrhea, gastroenteritis
Auscultation of Abdomen • Vascular sounds • use bell over vascular landmarks • listen for bruits N = no audible bruits Abnormal Finding : bruit present indicating turbulent bld flow & parietal obstruction or stenosis • Venous hum • listen for venous hum in all 4 Quads N = not present Abnormal Finding : continuous pulsating sound in periumbilical area dt portal obstruction caused by HPTN • Friction rubs • listen for rub over R & L costal margins, liver, spleen N= no rub heard (dt inflammation, tumors if heard)
Percussion • Percuss all four quadrants • Assess liver span, liver descent, margins of spleen, stomach, kidneys, liver, bladder • Sounds heard: tympany or dullness
Percussion of Abdomen • Percuss all four quads N= Tympany heard over air-filled areas, such as stomach and intestines N = Dullness heard over solid areas, such as liver or a distended bladder • Abnormal Findings : • Dullness over areas where tympany is normally heard may indicate a mass or tumor, pregnancy, ascites, full intestine
Percussion of Abdomen • Assess liver span • percuss upwards from umbilicus to lower border of liver on R midclavicular line • mark where sound chgs • percuss from lung to upper liver border R midclavicular line N= no tenderness, 6-12 cm btwn lines or • Scratch Test using stethoscope • Place stethoscope on R midclavicular line and scratch RLQ q 1-2 cm towards stethoscope …when you reach the lower border the sound will be louder. • Abnormal Findings • Liver span > 12 cm or < 6 cm • May indicate hepatomegaly or cirrhosis
Percussion of Abdomen • Percuss the Spleen • Percuss the lower level of the L lung posterior to the midaxillary line • Percuss downwards until dullness is heard N= splenic dullness heard from the 6th to 10th rib approx 6-8 cm above the L costal margin Abnormal Findings: Spleen dullness > 8 cm line May indicate splenic enlargement
Percussion of Abdomen • Percuss Stomach • Percuss for gastric air bubble • LUQ at L lower anterior rib cage and L epigastric region N = tympany of gastric bubble is lower in pitch that of intestines
Fist Percussion • Kidney • Direct method • Indirect method N= No tenderness • Abnormal Findings: • Costovertebral angle tenderness may indicate pyelonephritis
Fist Percussion • Liver • Indirect method • R lower rib cage N= No tenderness • Abnormal Findings: • Pain indicates cholecystitis or hepatitis
Percussion of Abdomen • Bladder • Percuss upwards from symphysis pubis to umbilicus • Note sound changes form dullness to tympany N =Urine filled bladder is dull to percussion =Empty bladder is not percussable above the symphysis pubis Abnormal Findings: Ability to percuss a recently emptied bladder may indicate urinary retention
Palpation of Abdomen • Palpate all 4 quadrants • Light vs. deep N= No tenderness, Smooth with consistent softness, No muscle guarding Abnormal Findings: • Tenderness on palpation • May indicate inflammation, masses, or enlarged organs • Muscle guarding on expiration • May indicate peritonitis • Presence of masses, bulges, or swelling • May indicate enlarged organs, cholecystitis, hepatitis, cirrhosis
Deep Palpation of Abdomen • One hand Method Bimanual Method
Assessing for Ascites • Fluid Wave Test • Position pt supine • Firmly place ulnar side of hand midline on abdomen to prevent displacement of fat • Place hand on pt’s R hip or flank area • Deliver a blow to pt’s L hip or flank area N= no fluid wave felt • Abnormal Findings: • Presence of fluid wave = ascites
Assessing the Liver • Bimanual Method • Hook Method N= liver edge presents firm sharp regular ridge • Abnormal Findings: • Liver is palpable below costal margin • May indicate CHF, hepatitis, cirrhosis, encephalopathy, cancer • Enlrged liver
Assessing for Cholecystitis • Murphy’s Sign • Palpate below the liver margin at lateral border • Have pt take deep breath • N= no pain elicited • Abnormal Finding: • Pt stops inhaling to guard against pain indicates a +ve Murphy’s sign = inflammation of gallbladder dt cholecystitis
Assessing the Spleen • Bimanual Method • Reach over pt and place L hand under rib cage, lift upwards • R hand deeply palpates • Ask pt to take deep breath N= the spleen is not palpable • Abnormal Findings: • Spleen is palpable • May indicate inflammation, CHF, cancer, cirrhosis, mononucleosis
Assessing the Kidneys • Bimanual Method N = kidneys are not palpable • Abnormal Findings: • Kidneys are palpable • May indicate hydronephrosis, neoplasms, polycystic kidney disease
Palpation of the Arota • Press the upper abdomen with one hand on either side of the aorta N= aorta width is 2.5-4 cm • Abnormal Findings: • Aorta width > 4 cm May indicate abdominal aortic aneurysm
Assessing for Abdominal Inflammation • Rebound Tenderness “Mc Burney’s Point” • Apply firm pressure at 90° in RLQ for 5 secs • Quickly release N= no pain in McBurneys point • Abnormal Findings: • Pain in RLQ indicates appendicitis
Assessing for Appendicitis • Rovsing’s Sign • Press firmly in LLQ for 5 secs • Note pts response N= no pain elicited • Abnormal Findings: • Pain in RLQ indicates appendicitis • +ve Rovsing’s Sign
Assessing the Bladder • Deep palpation • Midline starting at symphysis pubis upward to umbilicus N = empty bladder is not palpable Full bladder= smooth & round Abnormal Findings: • Able to palpate recently emptied bladder • May indicate urinary retention
Assessing Lymph Nodes • Pt supine , knees slightly flexed • Palpate lymph nodes in R & L inguinal area N= palpable non- tender small, movable nodes <1cm in diameter • Abnormal Findings: • Palpable inguinal lymph nodes > 1 cm in diameter or tender • May indicate systemic infections, cancer
Gerontological Variations • Abdominal musculature diminishes in mass and tone • Increased fat deposition in abdominal area • Altered GI motility results in changes in digestion and absorption • Decreased secretion of gastric acid • Increased incidence of malignant disease • Changes in bowel habits