Download
1 / 47
521 likes | 2.04k Views
EFFECT OF MATERNAL DRUGS ON FETUS. Congenital Malformations. 3-4% of all babies are born with a major birth defect Of these, 50% are of unknown cause Consider teratogen exposure and realize genetics plays a role. TERATOGENS.

E N D
Congenital Malformations • 3-4% of all babies are born with a majorbirth defect • Of these, 50% are of unknown cause • Consider teratogen exposure andrealize genetics plays a role
TERATOGENS • A substance, organism, physical agents or deficiency state capable of inducing abnormal structure or function such as: • Gross structural abnormalities • Functional deficiencies • Intrauterine growth restriction • Behavioral aberrations
Teratogenic agents • 1) Drugs and chemicals • 2) Infectious agents • 3) Radiation • 4) Other
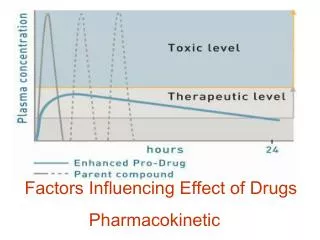
Teratogenic Factors • Time of exposure • Developmental stage during exposure • Maternal dose and duration • Maternal pharmacokinetics • Genetic factors/phenotypes • Interactions between agents
Drug Transfer to the Fetus Placental transfer may occur by: • Passive diffusion • Facilitated diffusion • Active transport • Placental surface area • Placental metabolism
Drug use in pregnancy Drugs can be harmful for the unborn fetus • Across Placenta • Molecular weight • Lipid solubility • Ionization • Protein binding • Chemical Structure
Fetal Drug Disposition • 60 – 80% passes through liver, the rest travels through ductus venosus to heart and brain • Hepatic drug metabolism • Adrenal gland metabolism • Recirculation through amniotic fluid
Drug use in pregnancy • Effects of toxic drugs• malformation• growth retardation• fetal death• functional defects in newborn• premature birth
Risk classifications • Different risk classifications have been proposed.• The FDA risk classification is widely usedRisk classification of FDAdrug risks to the fetus runs from:Category A (safest) → Category X (known danger--do not use!)
FDA Risk Categories A- Studies on humans; no risk B- Animal studies- no risk; No human studies C- Either animal studies show adverse effect and no human studies or no animal or human studies (benefit should outweigh risk) Drugs should be given only if the potentialbenefit justifies the potential risk to the fetus.
FDA Categories (cont) D- Positive evidence of human risk(drug is needed in a life-threatening situation orfor a serious disease for which safer drugs cannotbe used or are ineffective). X- Positive evidence of human risk; risk outweighs benefit and drug is contraindicated Thalidomide, DES (diethylstilboestrol). ,
Penicillins Cephalosporins Carbapenems Fluoroquinolones Macrolides Aminoglycosides Sulfonamides Antivirals Antiretrovirals Antifungals Anti-infectives
Penicillins Category B in pregnancy Cross the placenta easily and rapidly Concentrations increased in maternal levels
Cephalosporins Category B in pregnancy • Cross the placenta during pregnancy • Some reports of increased anomalies with specific cephalosporins (cefaclor, cephalexin, cephradrine) • Primarily cardiac and oral cleft defects
Carbapenems(ertapenem, imipenem, meropenem) • Category B/C/B in pregnancy • Likely cross the placenta • Very little human data
Fluoroquinolones(floxins) • Pregnancy Category C • Not recommended in pregnancy • Cartilage damage
Macrolides(azithromycin, clarithromycin, erythromycin) • Pregnancy Categories B/C/B • Cross the placenta in low amounts • Limited data with azithromycin and clarithromycin
Aminoglycosides(amikacin, gentamicin, tobramycin) • Pregnancy Category C Rapidly cross placenta Enter amniotic fluid through fetal circulation
Sulfonamides • Pregnancy Category C • Readily cross the placenta • Concerns of use at term
Antiepileptics • Risk for syndrome 10% • Dilantin- phenytoin syndrome • Microcephaly • Nail dysplasia • Developmental delay • Risk for some adverse effect (low IQ)- 30%
AccutaneX • Vitamin A derivative • Retinoic acid • Timing is key- beyond • 15 days postconception • Dose specific
Accutane • Risk of syndrome- 10-30% • Microcephaly/hydrocephaly • CHD • Microtia • Cleft lip/palate • Risk of spontaneous abortion- 25% • Risk of stillborn
Anticoagulants • Warfarin: D • Exposure- 4-7 weeks • Fetal warfarin syndrome: 10% • Hemorrhage • Depressed nasal bridge • Spontaneous abortion / stillbirth- 25%
Heparin • Not teratogenic
Angiotensin-converting enzymeinhibitor D • Reduced fetal renal blood flow • Fetal anuria • IUGR • Oligohydramnios
Tetracyclines • Maternal- • IV use in pregnancy: acute fatty liver, • hepatotoxicity • decidual bone/teeth: forms a complex calcium orthophospphate complications • Minor anomalies?
Quinolone • Animal studies • Fetal death, neonatal death, preterm delivery, IUGR • Anomalies: nonspecific • 1000 exposed women: no increase in adverse effects • Birth Registry: No increased risk • Use alternatives:
Lithium • 11% malformations rate- 1st trimester exposure • Most were CV defects • Risk of rare Ebstein’s anomaly • Neonatal toxicity (1-2 weeks)
Antivirals(acyclovir, famciclovir, valacyclovir) • Pregnancy Category B • Acyclovir and valacyclovir readily cross the placenta • Can be used for HIV treatment and suppression
Antiretroviralszidovudine • Pregnancy Category C • Maternal benefit usually outweighs fetal risk • Cross the placenta by simple diffusion • Zidovudine is commonly used, but may cause neonatal anemia
Antiretrovirals( nevirapine) • Pregnancy Category C • Maternal risk usually outweighs fetal risk • Likely cross into fetus Nevirapine can cause hepatotoxicity and rash • Nevirapine can be used as a single dose in labor to prevent HIV transmission
Antifungals/Azoles (fluconazole, ketoconazole) • Pregnancy Categories C/D • Likely cross placenta • Fluconazole > 400mg/day seems to be associated with cranio-facial abnormalities • Ketoconazole can impair cortisol synthesis
Ergots(Dihydroergotamine, ergotamine) • Pregnancy Category X • Oxytocic properties could cause IUGR by vascular disruption or increased uterine tone • Early exposure appears safe, not teratogens • Chronic exposure is contraindicated
Frequently used teratogenic agents • Alcohol• Smokingorofacial clefts 1/500 – 1/183lower birth weightpremature birth
Alcohol • 1-2% women of child-bearing age have an alcohol abuse problem • Fetal alcohol syndrome- most common cause of mental retardation in the US • Craniofacial skeletal abnormalities growth retardation mental disorders
Nicotine is a Neuroteratogen • Cell damage and deficits in cell number • Impaired synaptic activity • Receptor-Mediated, therefore low threshold • Affects Cell Replication/Differentiation Switchover • Initiates the Program for Cell Death • Morphological changes subtle but detectable in adulthood
Maternal Cigarette Smoking Maternal-Fetal Unit Nicotine in Fetus Effects on Fetal Brain General Development Hypoxia/Ischemia CO, HCN Anorexia Risky Behaviors: Other drugs/alcohol Prenatal Care Socioeconomic Perinatal Morbidity/Mortality Growth Retardation Behavioral Anomalies
Frequently used teratogenic agents • Coffee > 300 mg caffein/day (>3-6 cups of coffee) ↑ risk of fetal death advice: limit coffee to 3 cups/day • Vitamin A teratogenic in animal model, in human beings? avoid > 3 mg = 10.000 IE liver contains large amounts of vitamin A
Herbs use in pregnancy • Herbs not recommended nettle root• alkaloid-containing herbscoffee, mandrake (podophyllin) …• essential oilsrosemary …• anthraquinone laxativessenna …• herbs with potential hormonal actionhops, ginseng, licorice …
Drug use in pregnancy • Use of drugs in pregnancy is not always wrong • Drugs should be used with caution during pregnancy