Download
1 / 16
180 likes | 497 Views
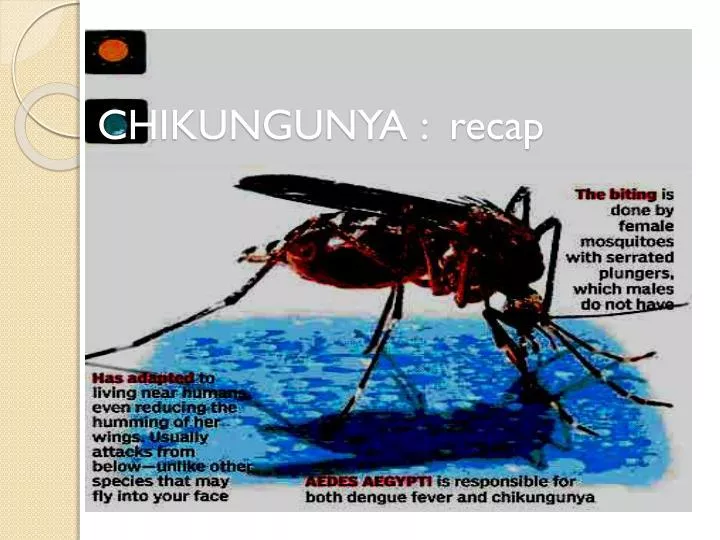
CHIKUNGUNYA : recap. EPIDEMIOLOGY. Epidemics of fever, rash and arthritis, resembling Chikungunya fever have been recorded as early as 1824 in India . Chikungunya fever displays interesting epidemiological profiles: major epidemics appear and disappear cyclically.

E N D
EPIDEMIOLOGY • Epidemics of fever, rash and arthritis, resembling Chikungunya fever have been recorded as early as 1824 in India . • Chikungunya fever displays interesting epidemiological profiles: major epidemics appear and disappear cyclically. • CHIK fevers have appeared in Indonesia in 1999. • Chikungunya in Asia and Africa (1960-1982) • Recent occurrences of chikungunya fever After an interval of more than 20 years, chikungunya fever has been reported from several countries including India, Indonesia, Maldives, Thailand • Chikungunya fever in India Till 10 October 2006, 151 districts of eight states/provinces of India have been affected by chikungunya fever. More than 1.25 million cases have been reported from the country with 752,245 cases from Karnataka and 258,998 from Maharashtra provinces. • Chikungunya and dengue fevers The clinical manifestations of chikungunya fever have to be distinguished from dengue fever. Co-occurrence of both fevers has been recently observed in Maharashtra state of India thus highlighting the importance of strong clinical suspicion and efficient laboratory support.
CHIKUNGUNYA in Malaysia – the little known virus SITI WAN ARIFAH BINTI WAN ABU HANIPAH SITI ZULAIHA ABU BAKAR
SPECIFICATION OF PROBLEM • While most of us were distracted by events of the world, this disease has steadily made its impact, not only in tropical regions but also in far-flung countries like Italy. • In Malaysia alone, in 2008, more than 3700 cases have occurred. It used to have an incidence of 100 cases per year but this has now risen to 100 cases per week. • Strangely enough, mainstream media has been deafeningly quiet and the health authorities have not done enough to educate the public on this relatively unknown condition. – press
History of Chikungunya‘development’ reported in malaysia • 1998 -1999 : first clinical disease outbreak in suburb of Klang , more than 51 persons infected • 2006 : BaganPanchor , Perak ; outbreak after 7 years , at least 200 cases reported, coincided with reports of ongoing epidemics in India and almost all the island nations of the Indian Ocean, with >200,000 cases in the French island of Reunion alone since February 2005 • 2008 : reemerging of endemic in Johor Bahru, more than 1000 suspected cases coincided with cases reported in Singapore • 2009 : 3988 cases reported positive (until October ) • 2010 : 787 cases reported positive (until October) after government launched the ‘War Against Dengue and Chikungunya’ like campaign
Quick facts on Chikungunya What is Chikungunya ? : Chikungunya (in the Makonde language "that which bends up") virus (CHIKV) is an insect-borne virus, of the genus Alphavirus, that is transmitted to humans by virus-carrying Aedesmosquitoes.[ Signs & Symptoms – • Sudden onset of high fever • Redness with rashes appearing on the hand, leg and body • Headache • Severe joint pains • Nausea and vomiting • Redness of the eyes • Fever can occur for a period from 1 - 7 days (usually 5 days) • (Commonly mistaken for dengue fever)
Quick facts on chikungunya • Incubation Period : Ranging from 3 - 12 days, usually 3 - 7 days • Care & Treatment : No specific treatmenttreated symptomatically (treating for specific symptoms) Majority need only outpatient treatment • Vaccine : No vaccine • Immunity : Most patients who have been infected will be immune for life. • Is it Contagious? - It is not contagious, in other words one human can't directly pass to another human. However an aedes mosquito after biting an infected person can transmit the disease by biting someone else
PATHOGENESIS • The virus is transmitted from human to human by the bites of infected female mosquitoes. Aedesaegypti and Aedesalbopictus. • After the bite of an infected mosquito, onset of illness occurs usually between four and eight days but can range from two to 12 days. • Both Ae. aegypti and Ae. albopictus have been implicated in large outbreaks of chikungunya. Whereas Ae. aegypti is confined within the tropics and sub-tropics, Ae. albopictus also occurs in temperate and even cold temperate regions. In recent decades Ae. albopictus has spread from Asia to become established in areas of Africa, Europe and the Americas. • The species Ae. albopictus thrives in a wider range of water-filled breeding sites than Ae. Aegypti. • This diversity of habitats explains the abundance of Ae. albopictus in rural as well as peri-urban areas and shady city parks. Ae. aegypti is more closely associated with human habitation and uses indoor breeding sites.
Aedesaegypti and Aedesalbopictus both species are found biting outdoors, but Ae. aegypti will also readily feed indoors found biting throughout daylight hours peaks of activity in the early morning and late afternoon the species Ae. albopictus thrives in a wider range of water-filled breeding sites than Ae. aegypti
Water-filled breeding sites saucers beneath plant pots vehicle tyres coconut husks cocoa pods tree holes bamboo stumps
Dengue and Chikungunyaawareness campaign • Aedes mosquito clearing operation when there was a cluster infection in a particular area. • Fogging and cleanliness activities especially in residential areas . • 1.2 million spent on mass media during first two weeks of campaign . • Flyers and pamplets distributions . • Checking the cleanliness on potential spots such as recreational spots, shopping malls, food courts, terminals for LRT, bus and taxi as well as tourists destinations . • Fines for ‘breeding’ aedes .
PREVENTION & CONTROL • No vaccine is available against this virus infection. • To avoid mosquito bites: Wear full sleeve clothes and long dresses to cover the limbs; Use mosquito coils, repellents Use mosquito nets – to protect babies, old people and others, who may rest during the day.
To prevent mosquito breeding Draining water from coolers, tanks, barrels, drums and buckets, etc.; Emptying coolers when not in use; Removing from the house all objects, which have water collected in them Cooperating with the public health authorities in anti-mosquito measures. • Role of public health authorities National programme for prevention and control of vector borne diseases should be strengthened Legislations for elimination of domestic/peridomesticmosquitogenic sites should be effectively enforced Communities must be made aware of the disease and their active cooperation in prevention and control measures elicited
Minimizing Transmission of Infection: This can be done in the following ways: • 1. Risk Communication to the household members: • Educate the patient and other members in the household about the risk of transmission to others and the ways to minimize the risk by minimizing vector population and minimizing the contact with vector. • 2. Minimizing vector population: • Intensify effort to reduce larval habitats in and around the houses: remove stagnant water from all junk items lying around and in the household and in the peri-domestic areas • Stagnating water in flower pots or similar containers should be changed daily or at least twice weekly • Introduce larvivorous fish in aquaria, garden pools, etc • Weeds and tall grasses should be cut short to minimize shady spaces where the adult insects hide and rest during hot daylight hours • Drain all water stagnating after rains • Fogging and street sanitation with proper waste management(fogging does not appear to be effective, yet it is routinely implemented in epidemic situation • 3. Minimize the vector-patient contact (Aedes mosquitoes bite during the daytime, mostly in the morning and late afternoon) • At household level: • Have the patient and infants in the house rest under bed-nets, preferably permethrin-impregnated nets • Insecticide sprays: bed rooms, closets and crevices, bathrooms, kitchens, nooks and corners; alternatively, coils , mats, vapourizers, etc • Have the patient as well as other members of the household wear full sleeves to cover extremities, preferably bright coloured clothes • Wire-mesh/nets on doors and windows • 4. Reporting to the nearest public health authority: • Occurrence of the case in the community needs to be communicated immediately to the nearest public health official for identification of clusters by person, place and time and for expansion of the control measures in the community and district levels.
REFERENCES • http://www.searo.who.int/en/Section10/Section2246.htm • http://www.medterms.com/script/main/art.asp?articlekey=3334 • http://www.homeopathyhelps.com/chikungunya.htm • http://www.chikungunia.com/ • http://www.who.int/mediacentre/factsheets/fs327/en/index.html • http://www.itsahealthguide.com/c3/p112/chikungunya_virus.html • http://moh.gov.my/ • http://www.ncbi.nlm.nih.gov.ezproxy.is.cuni.cz/pmc/articles/PMC2725805/ • http://doctor2008.wordpress.com/2009/01/11/health-alert5-this-thing-called-chikungunya/ • http://www.e-mjm.org/2009/v64n3/chikungunya.pdf • http://globalvoicesonline.org/2009/02/05/malaysia-war-on-dengue-and-chikungunya/ • http://daddy-o-ramblings.blogspot.com/2009/01/war-on-dengue-chikungunya.html • http://www.cdc.gov/eid/content/15/8/1243.htm • http://search.medscape.com/medscape-search?queryText=chikungunya