Download
1 / 28
280 likes | 411 Views
Screening & brief alcohol interventions in primary care. Dr Eileen Kaner Dr Paul Cassidy Professor Nick Heather Session 2 – Brief Alcohol Intervention. Linking screening to brief intervention. Avoid labelling Start with reference to the patient’s screening score or consumption level

E N D
Screening & brief alcohol interventions in primary care Dr Eileen Kaner Dr Paul Cassidy Professor Nick Heather Session 2 – Brief Alcohol Intervention
Linking screening to brief intervention • Avoid labelling • Start with reference to the patient’s screening score or consumption level • Ask the patient how they feel about their screening score/consumption level • eg. You appear to be drinking at a rate that increases your risk of harm. What do you think? • eg. The way in which you are drinking may be affecting your health. What do you think?
Assessing interest/motivation Not all patients are the sameAlcohol may not be at the top of their agenda
Stage of change & brief intervention • Precontemplation (unaware/unready) • intervention unlikely to succeed, give information about risks • Contemplation (aware/ambivalent) • offer advice &/or motivational work to move patient along • Preparation (planning) • set date, make plans, be specific, anticipate difficulties • Action (ready to go) • encourage, support, offer to follow-up • Maintenance (keeping it up) • reinforce success, advise on managing slips/relapse prevention
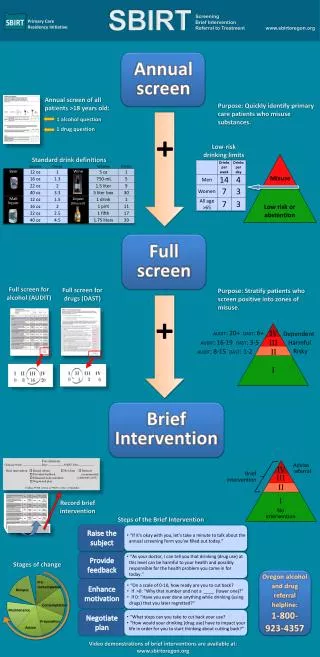
Risk status & brief intervention • Low Risk - Brief congratulation, positive reinforcement. Possibly ‘unit awareness’ work. • Hazardous drinkers – Simple structured advice (level 1 BI), offer further support • Harmful drinkers – Simple structured advice (level 1 BI) and offer motivational intervention (level 2 BI) • Dependent drinking – Referral to specialist services
Level 1 brief intervention • Simple structured advice • Delivered in 1-2 minutes • Following ‘How Much is Too Much’ protocol (level 1) • Practical - ‘common sense’ content • Offer of future follow-up/further discussion • Clinicians already do many elements of BI • just needs some more structure
BI structure – FRAMES • Feedback (personalised) • Responsibility (with patient) • Advice (clear, practical) • Menu (variety of options) • Empathy (warm, reflective) • Self-efficacy (boosts confidence)
Discussion • Issues to think about • What are the essential elements if time is short? • When, where and by whom? • What resources are required • What if patients want more than simple advice?
Level 2 brief intervention • Motivationally enhanced intervention not MI • Behaviour change counselling based on Rollnick S., et al. (1999) Health Behaviour Change: A Guide for Practitioners • Following ‘How much is Too Much’ – level 2 • Takes 15-20 minutes • 2-3 hour skill-based training available - Dr Malcolm Thomas, Effective Professional Interactions (http://www.effectivepi.co.uk)
Motivational approach fits with patient centred practice • Both clinicians and patients are experts • Distinction between disease and illness • Understanding patients in a context • Finding common ground • Mutual decision making
Gathering information Parallel search of two frameworks Disease framework Illness framework Integration of the two frameworks Shared understanding & decision making Patient presents problem • Doctor’s agenda: • Symptoms • Signs • Investigations • Pathophysiology • Patient’s agenda: • Ideas • Concerns • Expectations • Feelings Understanding the patient’s unique experience of illness Differential diagnosis
Patient centred practice - active listening patient practitioner What I say What I hear What I understand What I mean or feel
This person ought to change this person wants to change patient’s health is motivation no change=failure either do or don’t Now is the right time being tough is best I know - my advice is good negotiation is always best Clinician assumptions
Motivational Interviewing • ‘client-centred , directive method for enhancing intrinsic motivation to change by exploring and resolving ambivalence’ 1. Express empathy 2. Develop discrepancy 3. Avoid argumentation 4. Roll with resistance 5. Support self-efficacy Miller & Rollnick 2002
Behaviour change counselling • ‘ways of structuring a conversation which maximises the individual’s freedom to talk and think about change in an atmosphere free of coercion and the provision of premature solutions’ Rollnick et al. 1999 • Assessing readiness • Weighing up pros and cons • Determining action - moving patients on Rollnick et al. 1999
Discussion • Issues to think about • How could this fit in PHC? • Who might be best place to deliver this? • In what context could it be offered? • How should it be incentivised • What about patients who need more?
Referral (1) • Patients should be referred to specialist services who: • show a relatively high level of alcohol dependence or alcohol-related harm • are harmful drinkers who have not benefited from brief counselling and wish to receive further help for their alcohol problems
Referral (2) • can be defined as score of 20+ on the full AUDIT • obvious signs of physical dependence (e.g. withdrawal symptoms, withdrawal relief or avoidance drinking, very high tolerance, blackouts) • severe alcohol-related problems or risk of such problems (e.g. possible loss of job, family, etc.) • score on recognised measure of dependence (e.g. 10-item Leeds Dependence Questionnaire)