Download
1 / 1
10 likes | 74 Views
WePeB5707. Prevalence of resistance mutations in a cohort of treatment-naïve people with chronic HIV infection in the U.S.: CPCRA 058

E N D
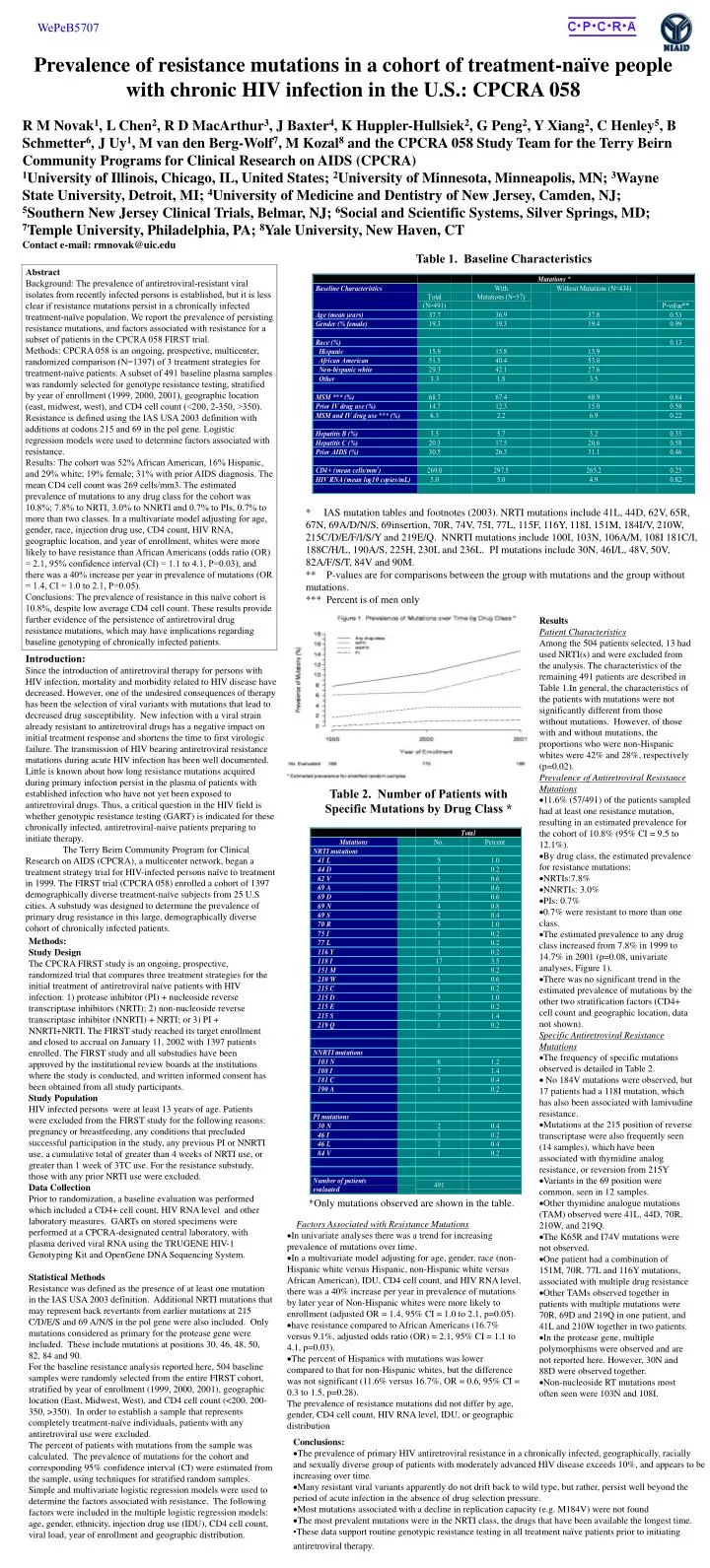
WePeB5707 Prevalence of resistance mutations in a cohort of treatment-naïve people with chronic HIV infection in the U.S.: CPCRA 058 R M Novak1, L Chen2, R D MacArthur3, J Baxter4, K Huppler-Hullsiek2, G Peng2, Y Xiang2, C Henley5, B Schmetter6, J Uy1, M van den Berg-Wolf7, M Kozal8 and the CPCRA 058 Study Team for the Terry Beirn Community Programs for Clinical Research on AIDS (CPCRA) 1University of Illinois, Chicago, IL, United States; 2University of Minnesota, Minneapolis, MN; 3Wayne State University, Detroit, MI; 4University of Medicine and Dentistry of New Jersey, Camden, NJ; 5Southern New Jersey Clinical Trials, Belmar, NJ; 6Social and Scientific Systems, Silver Springs, MD; 7Temple University, Philadelphia, PA; 8Yale University, New Haven, CT Contact e-mail: rmnovak@uic.edu Table 1. Baseline Characteristics Abstract Background: The prevalence of antiretroviral-resistant viral isolates from recently infected persons is established, but it is less clear if resistance mutations persist in a chronically infected treatment-naïve population. We report the prevalence of persisting resistance mutations, and factors associated with resistance for a subset of patients in the CPCRA 058 FIRST trial. Methods: CPCRA 058 is an ongoing, prospective, multicenter, randomized comparison (N=1397) of 3 treatment strategies for treatment-naïve patients. A subset of 491 baseline plasma samples was randomly selected for genotype resistance testing, stratified by year of enrollment (1999, 2000, 2001), geographic location (east, midwest, west), and CD4 cell count (<200, 2-350, >350). Resistance is defined using the IAS USA 2003 definition with additions at codons 215 and 69 in the pol gene. Logistic regression models were used to determine factors associated with resistance. Results: The cohort was 52% African American, 16% Hispanic, and 29% white; 19% female; 31% with prior AIDS diagnosis. The mean CD4 cell count was 269 cells/mm3. The estimated prevalence of mutations to any drug class for the cohort was 10.8%; 7.8% to NRTI, 3.0% to NNRTI and 0.7% to PIs, 0.7% to more than two classes. In a multivariate model adjusting for age, gender, race, injection drug use, CD4 count, HIV RNA, geographic location, and year of enrollment, whites were more likely to have resistance than African Americans (odds ratio (OR) = 2.1, 95% confidence interval (CI) = 1.1 to 4.1, P=0.03), and there was a 40% increase per year in prevalence of mutations (OR = 1.4, CI = 1.0 to 2.1, P=0.05). Conclusions: The prevalence of resistance in this naïve cohort is 10.8%, despite low average CD4 cell count. These results provide further evidence of the persistence of antiretroviral drug resistance mutations, which may have implications regarding baseline genotyping of chronically infected patients. • * IAS mutation tables and footnotes (2003). NRTI mutations include 41L, 44D, 62V, 65R, 67N, 69A/D/N/S, 69insertion, 70R, 74V, 75I, 77L, 115F, 116Y, 118I, 151M, 184I/V, 210W, 215C/D/E/F/I/S/Y and 219E/Q. NNRTI mutations include 100I, 103N, 106A/M, 108I 181C/I, 188C/H/L, 190A/S, 225H, 230L and 236L. PI mutations include 30N, 46I/L, 48V, 50V, 82A/F/S/T, 84V and 90M. • ** P-values are for comparisons between the group with mutations and the group without mutations. • *** Percent is of men only • Results • Patient Characteristics • Among the 504 patients selected, 13 had used NRTI(s) and were excluded from the analysis. The characteristics of the remaining 491 patients are described in Table 1.In general, the characteristics of the patients with mutations were not significantly different from those without mutations. However, of those with and without mutations, the proportions who were non-Hispanic whites were 42% and 28%, respectively (p=0.02). • Prevalence of Antiretroviral Resistance Mutations • 11.6% (57/491) of the patients sampled had at least one resistance mutation, resulting in an estimated prevalence for the cohort of 10.8% (95% CI = 9.5 to 12.1%). • By drug class, the estimated prevalence for resistance mutations: • NRTIs:7.8% • NNRTIs: 3.0% • PIs: 0.7% • 0.7% were resistant to more than one class. • The estimated prevalence to any drug class increased from 7.8% in 1999 to 14.7% in 2001 (p=0.08, univariate analyses, Figure 1). • There was no significant trend in the estimated prevalence of mutations by the other two stratification factors (CD4+ cell count and geographic location, data not shown). Specific Antiretroviral Resistance Mutations • The frequency of specific mutations observed is detailed in Table 2. • No 184V mutations were observed, but 17 patients had a 118I mutation, which has also been associated with lamivudine resistance. • Mutations at the 215 position of reverse transcriptase were also frequently seen (14 samples), which have been associated with thymidine analog resistance, or reversion from 215Y • Variants in the 69 position were common, seen in 12 samples. • Other thymidine analogue mutations (TAM) observed were 41L, 44D, 70R, 210W, and 219Q. • The K65R and I74V mutations were not observed. • One patient had a combination of 151M, 70R, 77L and 116Y mutations, associated with multiple drug resistance • Other TAMs observed together in patients with multiple mutations were 70R, 69D and 219Q in one patient, and 41L and 210W together in two patients. • In the protease gene, multiple polymorphisms were observed and are not reported here. However, 30N and 88D were observed together. • Non-nucleoside RT mutations most often seen were 103N and 108I. Introduction: Since the introduction of antiretroviral therapy for persons with HIV infection, mortality and morbidity related to HIV disease have decreased. However, one of the undesired consequences of therapy has been the selection of viral variants with mutations that lead to decreased drug susceptibility. New infection with a viral strain already resistant to antiretroviral drugs has a negative impact on initial treatment response and shortens the time to first virologic failure. The transmission of HIV bearing antiretroviral resistance mutations during acute HIV infection has been well documented. Little is known about how long resistance mutations acquired during primary infection persist in the plasma of patients with established infection who have not yet been exposed to antiretroviral drugs. Thus, a critical question in the HIV field is whether genotypic resistance testing (GART) is indicated for these chronically infected, antiretroviral-naive patients preparing to initiate therapy. The Terry Beirn Community Program for Clinical Research on AIDS (CPCRA), a multicenter network, began a treatment strategy trial for HIV-infected persons naïve to treatment in 1999. The FIRST trial (CPCRA 058) enrolled a cohort of 1397 demographically diverse treatment-naïve subjects from 25 U.S cities. A substudy was designed to determine the prevalence of primary drug resistance in this large, demographically diverse cohort of chronically infected patients. Table 2. Number of Patients with Specific Mutations by Drug Class * Methods: Study Design The CPCRA FIRST study is an ongoing, prospective, randomized trial that compares three treatment strategies for the initial treatment of antiretroviral naïve patients with HIV infection: 1) protease inhibitor (PI) + nucleoside reverse transcriptase inhibitors (NRTI); 2) non-nucleoside reverse transcriptase inhibitor (NNRTI) + NRTI; or 3) PI + NNRTI+NRTI. The FIRST study reached its target enrollment and closed to accrual on January 11, 2002 with 1397 patients enrolled. The FIRST study and all substudies have been approved by the institutional review boards at the institutions where the study is conducted, and written informed consent has been obtained from all study participants. Study Population HIV infected persons were at least 13 years of age. Patients were excluded from the FIRST study for the following reasons: pregnancy or breastfeeding, any conditions that precluded successful participation in the study, any previous PI or NNRTI use, a cumulative total of greater than 4 weeks of NRTI use, or greater than 1 week of 3TC use. For the resistance substudy, those with any prior NRTI use were excluded. Data Collection Prior to randomization, a baseline evaluation was performed which included a CD4+ cell count, HIV RNA level and other laboratory measures. GARTs on stored specimens were performed at a CPCRA-designated central laboratory, with plasma derived viral RNA using the TRUGENE HIV-1 Genotyping Kit and OpenGene DNA Sequencing System. Statistical Methods Resistance was defined as the presence of at least one mutation in the IAS USA 2003 definition. Additional NRTI mutations that may represent back revertants from earlier mutations at 215 C/D/E/S and 69 A/N/S in the pol gene were also included. Only mutations considered as primary for the protease gene were included. These include mutations at positions 30, 46, 48, 50, 82, 84 and 90. For the baseline resistance analysis reported here, 504 baseline samples were randomly selected from the entire FIRST cohort, stratified by year of enrollment (1999, 2000, 2001), geographic location (East, Midwest, West), and CD4 cell count (<200, 200-350, >350). In order to establish a sample that represents completely treatment-naïve individuals, patients with any antiretroviral use were excluded. The percent of patients with mutations from the sample was calculated. The prevalence of mutations for the cohort and corresponding 95% confidence interval (CI) were estimated from the sample, using techniques for stratified random samples. Simple and multivariate logistic regression models were used to determine the factors associated with resistance. The following factors were included in the multiple logistic regression models: age, gender, ethnicity, injection drug use (IDU), CD4 cell count, viral load, year of enrollment and geographic distribution. *Only mutations observed are shown in the table. • Factors Associated with Resistance Mutations • In univariate analyses there was a trend for increasing prevalence of mutations over time. • In a multivariate model adjusting for age, gender, race (non-Hispanic white versus Hispanic, non-Hispanic white versus African American), IDU, CD4 cell count, and HIV RNA level, there was a 40% increase per year in prevalence of mutations by later year of Non-Hispanic whites were more likely to enrollment (adjusted OR = 1.4, 95% CI = 1.0 to 2.1, p=0.05). • have resistance compared to African Americans (16.7% versus 9.1%, adjusted odds ratio (OR) = 2.1, 95% CI = 1.1 to 4.1, p=0.03). • The percent of Hispanics with mutations was lower compared to that for non-Hispanic whites, but the difference was not significant (11.6% versus 16.7%, OR = 0.6, 95% CI = 0.3 to 1.5, p=0.28). • The prevalence of resistance mutations did not differ by age, gender, CD4 cell count, HIV RNA level, IDU, or geographic distribution • Conclusions: • The prevalence of primary HIV antiretroviral resistance in a chronically infected, geographically, racially and sexually diverse group of patients with moderately advanced HIV disease exceeds 10%, and appears to be increasing over time. • Many resistant viral variants apparently do not drift back to wild type, but rather, persist well beyond the period of acute infection in the absence of drug selection pressure. • Most mutations associated with a decline in replication capacity (e.g. M184V) were not found • The most prevalent mutations were in the NRTI class, the drugs that have been available the longest time. • These data support routine genotypic resistance testing in all treatment naïve patients prior to initiating antiretroviral therapy.



















