Download
1 / 38
380 likes | 584 Views
Circulating Vitamin D Levels. Beth Zubal, MS, AOCNP, FNP-BC. D History…. 1822 – Sniadecki: Clinical observation of urban children with ↑rickets compared to rural children By 1900 , 80% of Boston children had rickets (pollution) 1930s , food fortified with Vitamin D,

E N D
Circulating Vitamin D Levels Beth Zubal, MS, AOCNP, FNP-BC
D History… 1822 – Sniadecki: Clinical observation of urban children with ↑rickets compared to rural children By 1900, 80% of Boston children had rickets (pollution) 1930s, food fortified with Vitamin D, Schlitz Brewery (Milwaukee, WI) introduced beer fortified with Vitamin D 1980, Coppertone developed UVA/UVB sunscreen Holick MF. VITAMIN D AND HEALTH IN THE 21ST CENTURY: BONE AND BEYOND. Sunlight and vitamin D for bone health and prevention of autoimmune diseases, cancers, and cardiovascular disease. Amer J Clin Nutr, Vol. 80, No. 6, 1678S-1688S, December 2004. Sniadecki J. Jerdrzej Sniadecki (1768–1838) on the cure of rickets (1840); cited in Mozolowski W. Nature 1939;143:121–4.
20,000 IU of Vitamin D < 30 min of sunlight 200 glasses of milk or 50 standard multivitamins (400IU/tab) in one sitting = Cannell, JJ, Hollis BW, Zasloff M et al. Diagnosis and treatment of Vitamin D deficiency. Expert Opin Pharmacother (2008) 9(1), 107-118.
Selected Food Sources of Vitamin D *IUs = International Units **DV = Daily Value Table from Office of Dietary Supplements: NIH. Retrieved January 15, 2009 http://ods.od.nih.gov/factsheets/vitamind.asp
Circulation • Vitamin D enters circulation through • Skin (D to D3) (Endogenous) • Diet (D3) (Exogenous) • Supplements • Vit D2-ergocalciferol • D3 - cholecalciferol • Prescription – Calcitriol (synthetic analog)
D Conversion: Liver converts to inactive 25 (OH)D (=calcitriol) by cytochrome P450 Kidney = “gets it going” 25(OH)D physiologically active to 1,25(OH)D most potent form of Vit D Parathyroid – stimulates synthesis 1,25(OH)D maintains calcium level
Parathyroid Hormone During hypocalcemia, responsible for: Mobilizing bone calcium Increasing reabsorption of calcium by kidneys Intestinal absorption of calcium
Definitions Normal level of 25-Hydroxy Vitamin D: > 30 ng/ml Insufficiency: 21 – 29 ng/ml Deficiency: < 20 ng/ml From: Holick (2008) Nutrition Reviews, Vol 66 (Suppl 2), S182-S194
Levels Associated with Disorders Prevention of rickets and osteomalacia 15 ng/ml Supression of parathyroid hormone 20 – 30 ng/ml Optimal intestinal absorption of calcium 34 ng/ml Neuromuscular function/performance 38 ng/ml Cannell, Hollis, Zasloff, & Heaney. (2008). Expert Opin. Pharmacother. 9(1): 107-118.
Serum 25-Hydroxyvitamin D [25(OH)D] Concentrations and Health * Serum concentrations of 25(OH)D are reported in both nanograms per milliliter (ng/mL) and nanomoles per liter (nmol/L).** 1 ng/mL = 2.5 nmol/L. Table from Office of Dietary Supplements: NIH. Retrieved January 15, 2009 http://ods.od.nih.gov/factsheets/vitamind.asp
Dosing Recommendations for Deficiency Insufficiency 800 – 1,000 IU of D³ daily Brings level to 30ng/ml in 3 months Deficiency Initial dose: 50,000 IU of D² or D³ po weekly for 6 – 8 weeks Subsequent dose: 800 – 1,000 IU of D³ daily Malabsorptive States Doses from 10,000 – 50,000 IU daily may be needed
Covered Diagnoses Hypocalcemia Persistent, nonspecific musculoskeletal pain Fatigue Those on anticonvulsant therapy Suspected toxicity
Factors Contributing to Decreased Levels Living in a northern latitude- > 35º Melanin content in skin Age: Elderly Obesity Use of sunscreen Clothing coverage Breast fed infants
Vitamin D Deficiency in the Elderly Vitamin D Deficiency AGE
Symptoms Associated with Vitamin D Deficiency Muscle weakness Myalgia Bone pain Nausea Hypocalcemia Hyperparathyroidism Osteopenia Fractures
Frequency of Testing At risk patients Check twice a year, once in early spring to determine lowest level and again in late summer for peak level. Those started on treatment Three months after therapy initiated
Drug Interactions with Vitamin D Steroids Anti-convulsants: phenytion Bile acid sequestrants: Questran Thiazide diuretics given to patients with hypoparathyroid on D2 may cause hypercalcemia Mineral oil effects absorption
Laboratory Tests for Vitamin D 25-Hydroxy Vitamin D 1,25-Dihydroxy Vitamin D Vitamin D panel: includes 25-Hydroxy and 1,25-Dihyroxy levels
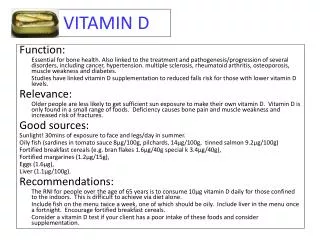
Functions of Vitamin D Promotes calcium absorption from gut Maintain adequate calcium and phosphate concentrations Modulates neuromuscular and immune function Reduces inflammation Has a role in cell proliferation, differentiation, and apoptosis
Consequences of Vitamin D Deficiency Holick, M. N Engl J Med, 2007;357:266-281; Wicherts et al. J Clin Endocrinol Metb. 2007;92:2058-2065. ; van Loden et al. Semin Oncol. 2008;35(6):643-651. • Skeletal • Osteoporosis • Osteomalacia and bone pain • Muscle weakness • Nonskeletal • Chronic disease: autoimmune diseases, osteoarthritis, diabetes • Cancer • Tuberculosis • Cardiovascular disease
Pharmacogenomics Nearly 200 human genes contain vitamin D receptors (1) (brain, pancreas, heart, GI tract, immune system, prostate, bones) Binding of VDR by calcitriol leads to multiple cellular effects: apoptosis, angiogenesis and potential of metastasis (2) • Carlberg C. Current understanding of the function of the nuclear vitamin D receptor In response to its natural and synthetic ligands. Recent Results Cancer Res. 2003; 164: 29-42. • Ng K, Meyerhardt, JA, Wu K, et. al. Higher pre-diagnosis plasma levels of serum 25-hydroxy-vitamin D (25[OH]D) after a diagnosis of colorectal cancer may significantly improve overall survival. J Clin Oncol 26(18), 2984-2991, 2008.
Fok1 polymorphism Tang C, Chen N, Wu M, et al. Fok1 polymorphism of vitamin D receptor gene contributes to breast cancer susceptibility. Breast Cancer Res Treat. Published online: 06 January 2009: DOI 10.1007/s10549-008-0262-4. • Vitamin D receptor (VDR) important role in Vitamin D pathway • May be greater in European women • Steroid family of nuclear receptors • More than 80% of breast cancers are VDR +
Breast Cancer 94% more likely to develop metastases and 73% more likely to die than women with normal levels of vitamin D at diagnosis Goodwin P. Frequency of vitamin D (Vit D) deficiency at breast cancer (BC) diagnosis and association with risk of distant recurrence and death in a prospective cohort study of T1-3, N0-1, M0 BC. American Society of Clinical Oncology Annual Meeting: Abstract 511. 2008.
Balance of Calcium Vitamin D balance is crucial for proper calcium utilization including: calcium absorption bone growth osteoclast/osteoblast activity
Bone Loss and Breast Cancer • Treatment with Aromatase Inhibitors (AIs) • Chemotherapy causing ovarian failure • Radiotherapy Hadji P, Body JJ, Aapro MS, et al. Practical guidance for the management of aromatase inhibitor-associated bone loss. Ann Onc 2008 Aug; 19(8): 1407-16. Epub 2008 Apr 29.
Vitamin D deficiency-incidence and response to oral supplementation among various gastrointestinal malignancies Gilmore C, James J, Zubal B, Thomas D, Tan B Washington University School of Medicine Siteman Cancer Center St. Louis, MO
Gilmore C, James J, Zubal B et al. Vitamin D deficiency-incidence and response to oral supplementation among various gastrointestinal malignancies. 2009 GI ASCO. Abstract No: 329.
Gilmore C, James J, Zubal B et al. Vitamin D deficiency-incidence and response to oral supplementation among various gastrointestinal malignancies. 2009 GI ASCO. Abstract No: 329.
Gilmore C, James J, Zubal B et al. Vitamin D deficiency-incidence and response to oral supplementation among various gastrointestinal malignancies. 2009 GI ASCO. Abstract No: 329.
Treatment • Pts with 25-OH Vitamin D level < 20-Vitamin D 50,000u q week x12 • Pts with 25-OH Vitamin D level 21-50-Vitamin D 50,000u q week x8 • Serum 25-OH re-checked after 8-12 weeks of therapy and if still <50 ng/ml continued on therapy according to above guideline • Goal to get 25-OH vitamin D level to 50 ng/ml and then maintain with 1000 to 2000u q day
Gilmore C, James J, Zubal B et al. Vitamin D deficiency-incidence and response to oral supplementation among various gastrointestinal malignancies. 2009 GI ASCO. Abstract No: 329.
Gilmore C, James J, Zubal B et al. Vitamin D deficiency-incidence and response to oral supplementation among various gastrointestinal malignancies. 2009 GI ASCO. Abstract No: 329.
Gilmore C, James J, Zubal B et al. Vitamin D deficiency-incidence and response to oral supplementation among various gastrointestinal malignancies. 2009 GI ASCO. Abstract No: 329.
Gilmore C, James J, Zubal B et al. Vitamin D deficiency-incidence and response to oral supplementation among various gastrointestinal malignancies. 2009 GI ASCO. Abstract No: 329.
Conclusions Vitamin D Deficiency is common among patients with GI malignancies. Vitamin D levels should routinely be evaluated for patients with GI malignancies. Oral supplementation decreases the rate of ‘any’ vitamin D deficiency from 81% to 61%, and of ‘severe to moderate’ deficiency from 58% to 17%. Prospective studies on the impact of vitamin D deficiency and supplementation on various clinical outcomes among patients with GI cancers would improve supportive care management of these patients.
Who should undergo serum testing? or Should we be asking, Who should not? ___________________________________________________