Download
1 / 29
290 likes | 297 Views
Learn about meningitis, an inflammation of the protective layers covering the brain and spinal cord, its causes, including bacterial and viral infections, and the importance of prompt medical attention and antibiotics.

E N D
What is meningitis?…… • The brain and spinal cord are covered by connective tissue layers collectively called the meninges which form the blood-brain barrier. 1-the pia mater (closest to the CNS) 2-the arachnoid mater 3-the dura mater (farthest from the CNS). The meninges contain cerebrospinal fluid (CSF). Meningitis is an inflammation of the meninges, which, if severe, may become encephalitis, an inflammation of the brain.
What is Meningitis? • Meningitis can be caused by many different organisms including viruses and bacteria. • Meningitis, caused by a bacteria, is life threatening and requires urgent medical attention and treatment with antibiotics. • Meningitis caused by a virus is very rarely life threatening but can cause the body to become very weak. • When bacteria invade the body they can cause meningitis, septicaemia or meningitis and septicaemia together
PACHYMENINGES/ LEPTOMENINGES • The inner two meninges, the arachnoid and the pia mater, between which circulates the cerebrospinal fluid. • The pachymeninges consist of the dura mater and outer layer of the arachnoid mater and cover the convex dural surface of the brain.
Causes of Meningitis -Bacterial Infections -Viral Infections -Fungal Infections (Cryptococcus neoformans Coccidiodes immitus) -Inflammatory diseases (SLE) Cancer -Trauma to head or spine.
Bacterial meningitis…..Etiological Agents: • Pneumococcal, Streptococcus pneumoniae (38%) • Meningococcal, Neisseria meningitidis (14%) • Haemophilus influenzae (4%) • Staphylococcal, Staphylococcus aureus (5%) • Tuberculous, Mycobacterium tuberculosis
N. meningitides G-ve diplococci E.Coli G-ve bacilli Streptococci-GBS G+ve cocci Strep. pneumoniae G+ve diplococci
Bacterial Meningitis Potentially life threatening disease. One million cases per year world wide. 200,000 die annually. Can affect all age groups but some are at higher risk. Treatment available : antibiotics as per causative organism Humans are the reservoir . Pneumococcal meningitis is the most common type. Approximately 6,000 cases/yr Haemophilus meningitis: Since 1985 Incidence has declined by 95% due to the introduction of Haemophilus influenza b vaccine. Other bacterial meningitis caused by E-Coli K-1, Klebsiella species and Enterobacter species are less common overall, but may be more prevalent in newborns, pregnant women, the elderly and immunocompromised hosts.
What is Meningococcal disease? Etiological Agent: Neisseria meningitidis Clinical Features: sudden onset. F,H,N,V Reservoir: Humans only. 5-15% healthy carriers Mode of transmission: direct contact with patients oral or nasal secretions. Saliva. Incubation period: 1-10 days. Usually 2-4 days Infectious period: as long as meningococci are present in oral secretions or until 24 hrs of effective antibiotic therapy Epidemiology: Sporadic cases worldwide. “Meningitis belt” –sub-Saharan Africa into India/Nepal. In US most cases seen during late winter and early spring. Children under five and adolescent most susceptible. Overcrowding e.g. dormitories and military training camps predispose to spread of infection.
Bacterial Meningitis - Pathogenesis • Infection of upper respiratory tract • Invasion of blood stream (bacteraemia) • Seeding & inflammation of meninges
Aseptic Meningitis Definition: A syndrome characterized by acute onset of meningeal symptoms, fever, and cerebrospinal fluid pleocytosis, with bacteriologically sterile cultures. Laboratory criteria for diagnosis: CSF showing ≥ 5 WBC/cu mm No evidence of bacterial or fungal meningitis. Case classification Confirmed: a clinically compatible illness diagnosed by a physician as aseptic meningitis, with no laboratory evidence of bacterial or fungal meningitis Comment Aseptic meningitis is a syndrome of multiple etiologies, but most cases are caused by a viral agent
Viral Meningitis Etiological Agents: Enteroviruses (Coxsackie's and echovirus): most common. -Adenovirus -Arbovirus -Measles virus -Herpes Simplex Virus -Varicella Reservoirs: -Humans for Enteroviruses, Adenovirus, Measles, Herpes Simplex, and Varicella -Natural reservoir for arbovirus birds, rodents etc. Modes of transmission: -Primarily person to person and arthopod vectors for Arboviruses Incubation Period: -Variable. For enteroviruses 3-6 days, for arboviruses 2-15 days Treatment: No specific treatment available. Most patients recover completely on their own.
Non Polio Enteroviruses Types:62 different types known: -23 Coxsackie A viruses, -6 Coxsackie B viruses, -28 echoviruses, and 5 other How common? -90% of all viral meningitis is caused by Enteroviruses -Second only to "common cold" viruses, the rhinoviruses. -Estimated 10-15 million/ more symptomatic infections/yr in US Who is at risk?Everyone. How does infection spread?Virus present in the respiratory secretions & stool of a patient. Direct contact with secretions from an infected person. Parents, teachers, and child care center workers may also become infected by contamination of the hands with stool.
The difference between Meningitis and Septicaemia When bacteria cause disease i.e. meningococcal disease the body can be affected in different ways: Meningitis - bacteria enter the blood stream and travel to the meninges and cause inflammation. Septicaemia - when bacteria are present in the blood stream they can multiply rapidly and release toxins that poison the blood. (The rash associated with meningitis is due to septicaemia.) Meningitis and septicaemia often occur together.
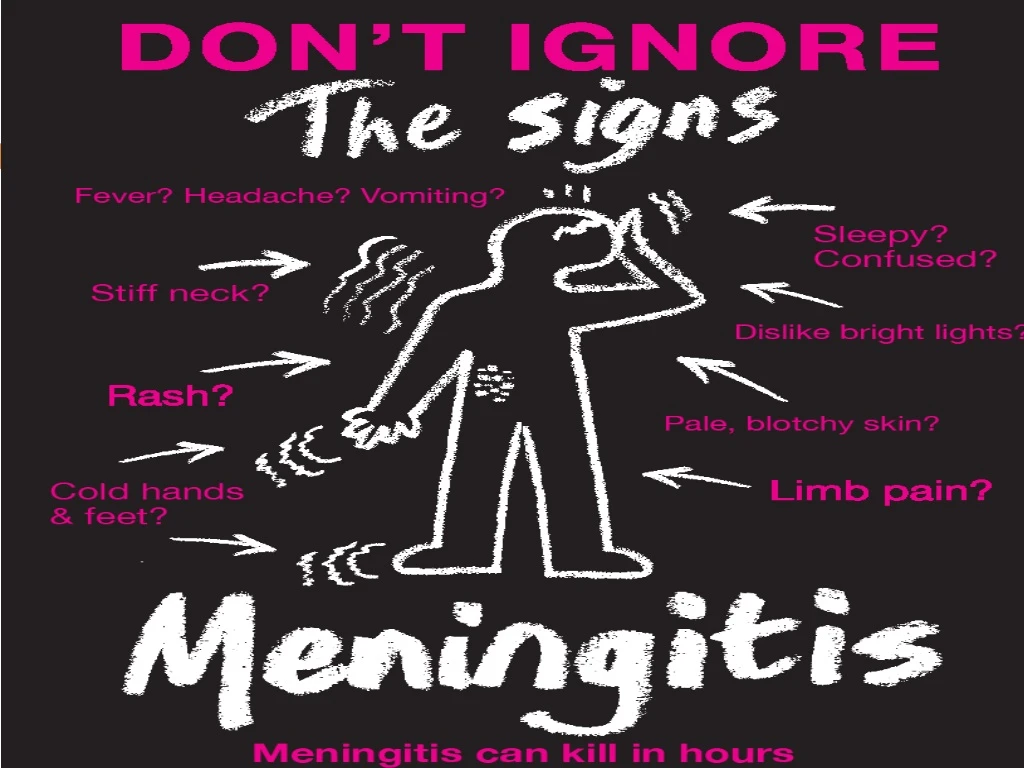
Symptoms for meningitis and meningococcal septicaemia: :Babies and Young Children -High temperature, fever, possibly with cold hands and feet -Vomiting or refusing feeds -High pitched moaning, whimpering cry -Blank, staring expression -Pale, blotchy complexion -Stiff neck -Arched back -Baby may be floppy, may dislike being handled, be fretful -Difficult to wake or lethargic -The fontanelle (soft spot on babies heads) may be tense or bulging.
Older Children and Adults -High temperature, fever, possibly with cold hands and feet. -Vomiting, sometimes diarrhoea. -Severe headache. -Joint or muscle pains, sometimes stomach cramps. -Neck stiffness (unable to touch the chin to the chest) -Dislike of bright lights. -Drowsiness. The patient may be confused or disorientated. A rash may develop.
One of the physically demonstrable symptoms of meningitis is Kernig's sign. Severe stiffness of the hamstrings causes an inability to straighten the leg when the hip is flexed to 90 degrees.
Another physically demonstrable symptoms of meningitis is Brudzinski's sign. Severe neck stiffness causes a patient's hips and knees to flex when the neck is flexed.
One sign of meningococcal septicaemia is a rash that does not fade under pressure (see ‘Glass test’) -This rash is caused by blood leaking under the skin. It starts anywhere on the body. It can spread quickly to look like fresh bruises. -This rash is more difficult to see on darker skin. Look on the paler areas of the skin and under the eyelids.
‘Glass Test’ A rash that does not fade under pressure will still be visible when the side of a clear drinking glass is pressed firmly against the skin. If someone is ill or obviously getting worse, do not wait for a rash. It may appear late or not at all. A fever with a rash that does not fade under pressure is a medical emergency.
Diagnosis LP
Antibiotics Less than 2 months of age: • Ampicillin + Cefotaxime+/- Gentamicin • Treat for 3 weeks (neonate) Over 2 months: • Cefotaxime • Treat for 7-10 days
Public Health Importance Challenges: -Educating public -Timely reporting and records keeping -Updating information daily. -Alleviating public anxiety and concerns -Collaborating with health partners Opportunities: -Educating public -Communication -Strengthening partnerships



















