Download
1 / 45
590 likes | 1.2k Views
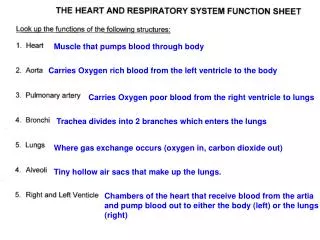
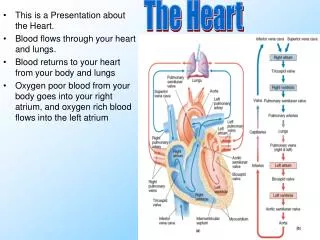
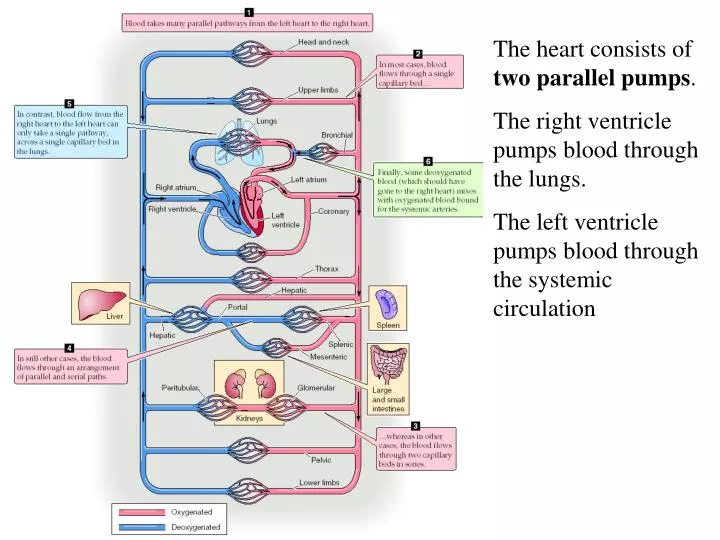
The heart consists of two parallel pumps . The right ventricle pumps blood through the lungs. The left ventricle pumps blood through the systemic circulation. Four valves cause one-way passage of blood through the two chambers of the heart. Mitral (inlet to the left ventricle)

E N D
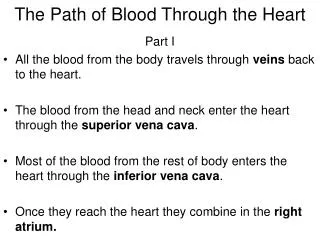
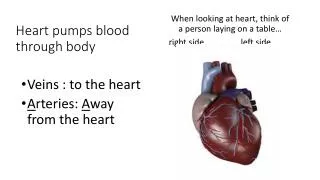
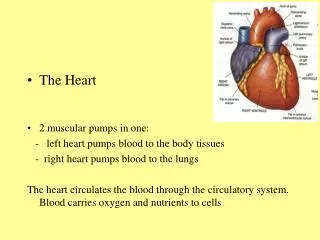
The heart consists of two parallel pumps. The right ventricle pumps blood through the lungs. The left ventricle pumps blood through the systemic circulation
Four valves cause one-way passage of blood through the two chambers of the heart. Mitral (inlet to the left ventricle) Tricuspid (inlet to the right ventricle) Aortic (outlet from the left ventricle) Pulmonic (outlet from the right ventricle)
The heart can be classified as a reciprocating type pump. Instead of a piston, however, the ventricular walls contract and relax to vary the volume of the lumen Unlike the pump shown here the heart does not suck blood into itself. All filling is under positive pressure as the venous pressure is required to stretch the muscle fibers.
During diastole there is passive filling of the relaxed left ventricle. The ventricle does not suck blood into the lumen. Filling is by the venous pressure.
The first sign of activity in the heart is the atrial contraction. This weak structure pushes a small amount of blood into the ventricle (atrial kick) Blood is also propelled back into the veins giving rise to the A-wave. Not vital.
Isovolumetric contraction occurs as the ventricle starts to contract. The mitral valve closes The ventricular pressure rises toward aortic pressure . The mitral valve bulges into the atrium causing the C wave in venous pressure
Ejection phase starts as the aortic valve opens. The ventricular contents are ejected during this time.
Isovolumetric relaxation begins as the aortic valve closes. Ventricular pressure falls from aortic to left atrial during this period.
Diastolic filling begins again as the mitral valve opens Accumulated blood in the atrium rushes into the ventricle Movement of blood into the ventricle causes venous pressure to drop suddenly causing the V wave
A common diagnostic technique is to place catheters at various points in the cardiovascular system and record their pressures.
There are 7 phases to the cardiac cycle • Atrial systole • Isovolumetric Contraction • Rapid Ejection • Reduced Ejection • Isovolumetric Relaxation • Rapid Filling • Reduced Filling (diastasis)
The difference between the peak and the trough is called the pulse pressure Blood pressure rises during systole and falls during diastole.
A is atrial systole. Causes the A wave in atrial pressure. Helps fill the ventricle.
B is Isovolumic contraction. It starts with mitral valve closure Both the aortic and mitral valves are closed so the ventricle’s volume is constant.
C is rapid ejection period. It starts with aortic valve opening. Ventricular pressure leads aortic. Flow out of the ventricle is accelerating.
D is the reduced ejection period. Aortic pressure leads ventricular. Flow out of the ventricle is decelerating.
E is the isovolumetric relaxation period. Begins with aortic valve closure. Ventricular volume is constant
F is the rapid filling period. Begins with opening of the mitral valve. Gives rise to the V wave as blood accumulated in the atrium rushes into the ventricle.
G is the reduced filling period. Ventricular filling is now in equilibrium with venous return.
Events on the right side are the same except the pressure is lower.
3/4 of the stroke volume occurs in the rapid ejection period The ventricle only ejects about ½ of its contents.
Left ventricular end-diastolic volume (LVEDV) Left ventricular end-systolic volume (LVESV) stroke volume= LVEDV-LVESV cardiac output = stroke volume x heart rate
Cardiac Work done is calculated as the volume it pumps times the pressure it pumps against. The left side does more work.
Since there are no valves between the atrium and veins atrial pressure is essentially equal to venous pressure. Notice the venous pressure trace with A, C and V waves
Two audible heart sounds: They are termed the first (S1) and second (S2). They sound like “lub dup”. The first is low pitched and the second is high. Sounds come from turbulent flow around the valve cusps and vibration of the heart structures
The first heart sound is complex 1. Regurgitant flow across the closing mitral valve. 2. Abrupt closure of mitral and tricuspid valves. 3. Opening of left and right semilunar valves. 4. Rapid acceleration of blood out of the ventricles
Second heart sound occurs at the end of systole and is due to closure of the two semilunar valves. The second heart sound is normally split because both valves do not always close simultaneously.
Normally the pulmonic valve is last to close. This is further delayed by inspiration
If splitting is enhanced on expiration it means that the aortic valve is closing last
Paradoxical splitting occurs with: things that delay left ventricular activation such as left bundle branch block
Things that weaken the left ventricle’s muscle such as left ventricular failure.
Two more sub-audible heart sounds are present, the third (S3) and fourth (S4) heart sounds.
Too faint to be heard but can be seen in a phonocardiogram If S3 or S4 are audible it is called a gallop.
S3 results from rapid filling of the ventricle during diastole. It is sometimes heard in normal children and in some patients with heart failure
Murmur is defined as a new cardiac sound unrelated to the four heart sounds. A murmur is generally caused by prolonged turbulent flow in either diastole or systole typically related to valvular stenosis or regurgitation but may also be caused by abnormal connections between right and left heart circulations.
The diastolic murmur of aortic regurgitation Decrescendo murmur blood pressure ECG
Pressure gradient The harsh systolic murmur of aortic stenosis The diagnosis is confirmed by demonstrating a pressure gradient across the aortic valve.
Things that raise pressure in the ventricle cause hypertrophy. The harsh systolic murmur of aortic stenosis
Thrill: a cardiovascular sound so intense that it can be felt with the fingers. This is commonly seen with the very loud murmur of patent ductus arteriosis.
Systolic murmurs • Mitral regurgitation • Aortic Stenosis • Diastolic murmurs • Mitral stenosis • Aortic Regurgitation • Continuous murmur • Patent Ductus