Download
1 / 62
620 likes | 693 Views
UGI Bleed. Obie M. Powell, M.D. Joseph A. Iocono, M.D. Department of Surgery University of Kentucky. Mr. Mellenna. 57 year-old white male with recent history of dark stools presents to the emergency room complaining of a two hour history of vomiting blood and feeling faint.

E N D
UGI Bleed Obie M. Powell, M.D. Joseph A. Iocono, M.D. Department of Surgery University of Kentucky
Mr. Mellenna 57 year-old white male with recent history of dark stools presents to the emergency room complaining of a two hour history of vomiting blood and feeling faint. On presentation the patient is pale and lethargic complaining of abdominal pain.
History What other points of the history do you want to know?
History, Mr. Mellenna Characterization of symptoms Temporal sequence Alleviating / Exacerbating factors: Pertinent PMH, ROS, MEDS. Relevant family hx. Associated signs and symptoms Consider the Following
Characterization of Symptoms Un-relenting nausea with associated burning epigastric discomfort Pain is steady and rates it as a 5 on a scale of 1-10.
Temporal Sequence Dark stools off and on for approximately 6 months. Often has some mild epigastric pain to which he pays little attention. This pain has been occurring for the same duration. Today he has been feeling “light headed” for about 3-4 hours, and has been throwing up blood for 2 hours.
Alleviating / Exacerbating Factors Standing erect worsens his light headedness and laying down improves it. Nothing improves the pain or nausea In the past eating food sometimes relieved his abdominal pain.
PMH The patients past history is significant for HTN MI 3 years prior treated with angioplasty and stenting. COPD Osteoarthritis No prior abdominal surgery
PMH Medications ASA - supposed to be on it but it bothers his stomach Metoprolol 50mg po BID Simvastatin 10mg po daily Ibuprofen 400mg po QID prn, none in past 2 weeks NKDA
Family/Social History Family History Non-contributory Social History Married Computer programmer ETOH- 6 pack per week
ROS As in HPI. The patient denies chest pain, shortness of breath, fever, chills, anorexia, and dysuria ROS should emphasize further characterization of the active disease process AND risk factors that may complicate surgery such as active infection, active CAD, poor exercise tolerance
Differential Diagnosis Esophageal varices Gastric varices Erosive gastritis Mallory Weiss tear Reflux esophagitis Gastric malignancy Vascular malformations Nose bleed Aorto-enteric fistula Gastric ulcer Duodenal ulcer Consider the following
Physical Exam What are you looking for?
Physical Exam What to look for Vital signs: instability, respiratory distress, beware of beta blockade Overall appearance: signs of anemia, dehydration Abdominal exam: probe for peritonitis Rectal exam: mandatory. Look for perianal causes of bleeding.
Physical Exam, Mr. Mellenna Vital signs: Temp. 97.8, Pulse 90, BP 95/63 Resp. 30 Patient is alert and oriented. Pale skin and dry mucous membranes. During your examination the patient has a large maroon bowel movement
Physical Exam Head is atraumatic / normocephalic, eyes sunken, pale conjunctiva Neck- No lymphadenopathy, flat neck veins. Oropharynx - dried blood, no active bleeding, dry mucus membranes. CV- Regular rate and rhythm, no murmur, rubs, or gallops Chest- Mild tachypnea, respirations are clear bilaterally no rales, rhonchi, or wheezes Abdomen is scaphoid, soft, mildly tender in mid-epigastrum. Bowel sounds are present and hyperactive. Extremities show no clubbing, cyanosis, or edema. Rectal exam shows gross blood, enlarged smooth prostate, no palpable masses, no hemmorhoids or other peri-anal disease
Would you like to revise your initial differential diagnosis?
Laboratory studies:What is necessary? Type and Cross CBC: Do you expect anemia? CMP: evaluate for hepatic dysfunction and renal compromise Coags: active hemorrhage can cause coagulopathy and requires aggressive replacement ABG: probe for acidosis
Laboratory Values 10.2 55 140 110 11 144 108 31.1 1.1 4.3 20 ABG: 7.23 | 28 | 80 | 18 | -5 PT: 18 (1.5) PTT: 36 LFTs: Normal
Laboratory Values Discussion An elevated BUN to Creatinine ratio can be a sign of upper GI bleed due to the digestion of blood or prerenal azotemia. A patient actively hemorrhaging will show a normal Hgb/Hct prior to being resuscitated. Chronic bleeding presents with typical iron deficiency anemia.
Interventions to consider ABC’s Ensure adequate airway protection and adequate respirations Start 2 large bore IV’s. Fluid bolus either NS or LR Foley Catheter NG with gastric lavage STAT Upper endoscopy
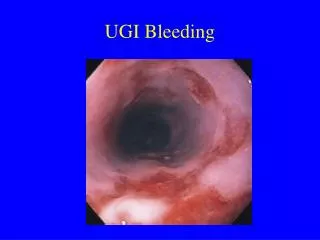
Endoscopy Upon upper endoscopy the esophagus appears normal. There is a large amount of clot in the stomach, irrigation reveals normal appearing mucosa without signs of ulcer or gastritis. On passing through the pylorus copious gross blood is encountered with a actively bleeding ulcer on the posterior wall of the duodenum.
Endoscopy Attempt at injecting with epinepherine, and even direct pressure prove unsuccessful with continued brisk pulsatile bleeding. Are there any particular endoscopic findings that suggest a higher risk of failed therapy or re-bleeding?
What would you do next? Repeat Hct is 18 He is actively bleeding in Endoscopy
Surgery for Bleeding Ulcers Indications Pre-operative preparation Operative approach Relevant Anatomy Potential complications
Operative Indications Duodenal ulcers located on the anterior wall are prone to perforation and present as peritonitis and free air. Those on the posterior wall, which is the more common location, lead to bleeding. The gastroduodenal artery passes just distal to the pylorus and posterior to the duodenum. If it or one of it’s branches are in the ulcer crater they may erode and result in massive bleeding.
Operative Technique Patients are explored through an upper midline incision. An incision is made in the anterior duodenum through the pylorus and distal stomach. The site of bleeding is identified. The bleeding can then usually be controlled by placing sutures in 3-4 quadrants around the ulcer base. The gastroduodenal artery may be ligated if necessary
Operative Technique Once bleeding has been controlled, the horizontal opening through the pyloric channel is closed vertically resulting in a Heineke-Mikulicz pyloroplasty. A truncal vagotomy is then added for long-term ulcer control. Specimens of both vagal trunks are sent to Pathology to document the vagotomy
Gastrointestinal Bleeding Discussion
Gastrointestinal Bleeding Bleeding can arise anywhere along the GI tract. Bleeding represents the initial symptom of gastrointestinal disease in 1/3 of all patients. The majority of bleeding will stop spontaneously.
Gastrointestinal Bleeding Hematemesis- Vomiting of blood. Can be either gross blood and blood clots representing rapid bleeding or “coffee-ground” emesis signifying chronic bleeding. Hematemesis is the result of bleeding from the oropharynx to the ligament of Treitz. Melena- Passage of black and tarry stool caused by digested blood.
Gastrointestinal Bleeding Melena is usually the result of severe upper GI bleeding. Melena without hematemesis is caused by severe bleeding distal to the ligament of Treitz. Hematochezia- Passage of maroon to red blood and blood clots.
Gastrointestinal Bleeding As little as 50-60 mL of blood in the GI tract produces melena. Melena can persist from 5-7 days after a 2 unit bleed and stools can remain occult positive up to 3 weeks. With upper GI blood loss blood urea nitrogen levels may be elevated to 30-50 mg/dL. A BUN: Creatinine ratio greater than 36:1 likely represents blood loss from an upper GI source.
Upper Gastrointestinal Bleeding Some dependency on socioeconomic factors. Peptic ulcers are more common in suburban hospitals, while gastritis and varices are more common in urban centers. Patients 60 years old and older represent ~ 60% of patients presenting with upper GI bleeding with a mortality rate of 20-25%. For younger patients the mortality rate drops to 4%.
Upper Gastrointestinal Bleeding Although elective surgeries for duodenal ulcers have dropped off significantly due to H2 blockers and proton pump inhibitors, the number of surgeries for bleeding duodenal ulcers has remained stable. Sudden cessation of H2 blockers or proton pump inhibitors may result in a rebound increase in acid secretion resulting in GI bleeding.
Upper Gastrointestinal Bleeding Nose bleeds- Rarely the cause of major bleeding. It must be ruled out by a careful examination of the posterior pharynx to insure blood is not running down the esophagus, causing hematemesis .
Upper Gastrointestinal Bleeding Esophagitis- Hiatus hernia and reflux esophagitis are not common causes of upper GI bleeding. Reflux esophagitis is more likely to result in chronic occult bleeding usually associated with grade II-III esophagitis with friable mucosa. Significant bleeding in this area is more commonly associated with para- esophageal hernias.
Upper Gastrointestinal Bleeding Varices- Bleeding esophageal and gastric varices in the presence of liver disease account for about 10% of upper GI bleeds and are life threatening situations associated with a high mortality rate. Alcoholism is the most common cause of portal hypertension but hepatitis B and C are becoming common causes.
Upper Gastrointestinal Bleeding Varices- In pediatric patients 95% of all upper GI bleeds are caused by variceal hemorrhage, usually as a consequence of extra hepatic portal venous obstruction. In patients with cirrhosis and portal hypertension variceal hemorrhage accounts for 50-75% of all upper GI bleeds. Variceal hemorrhage is usually precipitated by ulceration of the varix secondary to reflux esophagitis or increased pressure within the varix.
Upper Gastrointestinal Bleeding Varices- In patients with liver disease bleeding is precipitated by the inability of the liver to synthesize clotting factors. Initial therapy includes sclerotherapy, ligation and vasopressin. Ligation is as effective as sclerotherapy with fewer complications. If unsuccessful shunting or transplant may be necessary.
Upper Gastrointestinal Bleeding Mucosal tear (Mallory-Weiss) Esophagogastric mucosal tear or Mallory-Weiss tear account for 5-10% of all upper GI bleeds. Mallory-Weiss tears present in a classic pattern. Initially the patient has vomiting without blood. Continued emesis leads to pain from the tear and eventually the patient develops hematemesis. 90% of Mallory-Weiss bleeding resolves spontaneously and require no further therapy. If bleeding persists, endoscopic therapy with injection of vasoconstrictive agents, IV vasopressin or balloon tamponade with Sengstaken-Blakemoore tube may be necessary.
Upper Gastrointestinal Bleeding Gastritis Up to 1/3 of upper GI bleeds are caused by diffuse gastritis. Erosions are usually multiple and found primarily in the fundus and body of the stomach. Chronic slow bleeds are most commonly associated with H. pylori, while more brisk bleeding is usually a result of ingested substances harmful to the gastric mucosa such as NSAIDs, alcohol, steroids, or other drugs. Treatment is with vasopressin, iced saline lavage, sucralfate, H2 blockers, and proton pump inhibitors. Bleeds refractory to these treatments may require electrocautery, vagotomy and antrectomy or even total gastrectomy.
Upper Gastrointestinal Bleeding Peptic ulcer Most common cause of upper GI bleed, encompassing 1/2- 2/3 of patients. Bleeding is presenting symptom in up to 10% of these patients. Duodenal bleed is four times more common than gastric ulcer bleed. Duodenal ulcers are usually posterior and involve branches of the gastroduodenal artery. Benign gastric ulcers bleed more than malignant ulcers. There will be significant bleeding in 10-15% of peptic ulcers and surgical intervention is needed in 20% of these patients
Upper Gastrointestinal Bleeding Stress ulcers Stress ulcers refer to acute gastroduodenal lesions that arise after episodes of shock, sepsis, surgery, trauma, burns (Curling’s ulcer), or intracrainial pathology or surgery (Cushing’s ulcer). Specific risk factors associated with these ulcers are, multi system trauma, hypotension, respiratory failure, sepsis, jaundice, recent surgery and burns. It is believed that stress ulceration is the result of bile reflux damage to the gastric protective barrier combined with decreased gastric blood flow secondary to splanchnic vasoconstriction. Sepsis, coagulopathy, and activation of cytokines may also play a role in the formation of stress ulcers.
Upper Gastrointestinal Bleeding Other causes Miscellaneous causes may contribute up to 18% of upper GI bleeds. Gastric neoplasms both malignant and benign can cause bleeding which is usually mild and chronic. Dieulafoy’s vascular malformations are dilated arterial lesions usually amendable to endoscopic injection. Aorto-enteric fistulas can present as a herald bleed followed by a massive bleed in patients with prior aortic reconstructions. Hematobilia can be found in patients following hepatic injuries or manipulations.