Download
1 / 11
120 likes | 261 Views
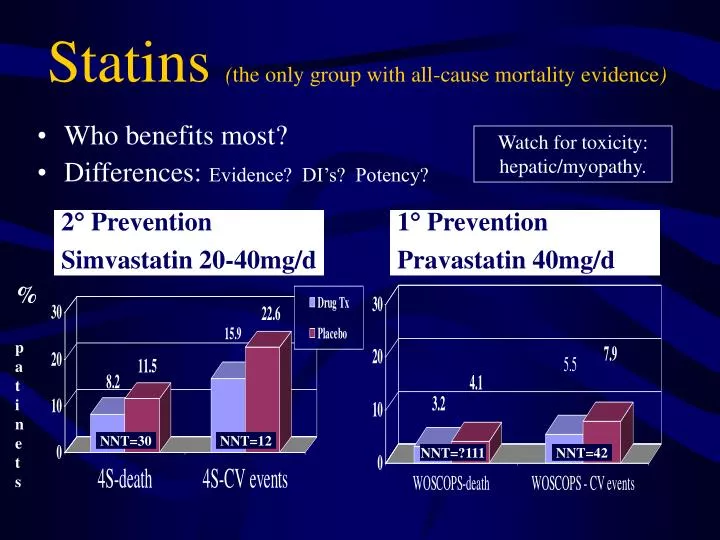
Who benefits most? Differences: Evidence? DI’s? Potency?. Statins ( the only group with all-cause mortality evidence ). Watch for toxicity: hepatic/myopathy. 2 Prevention Simvastatin 20-40mg/d. 1 Prevention Pravastatin 40mg/d. % patinets. NNT=30. NNT=12. NNT=?111. NNT=42.

E N D
Who benefits most? Differences: Evidence? DI’s? Potency? Statins (the only group with all-cause mortality evidence) Watch for toxicity: hepatic/myopathy. 2 Prevention Simvastatin 20-40mg/d 1 Prevention Pravastatin 40mg/d % patinets NNT=30 NNT=12 NNT=?111 NNT=42
HPS Lancet 2003 n=20,536 5yr Evidence for diabetes, stroke, age<80, women, LDL<3 • No benefit for Vitamins E 600mg, C 250mg, or beta-carotene • Questions remaining: safety/efficacy of aggressive pursuit of targets, combination therapies, low-risk patients with LDL. 2 & High-risk 1 Prevention (CHD, PVD, Diabetes, HTN, Male/Female, Age 40-80) Simvastatin 40mg/d Benefits similar despite lower vs higher initial LDL % patinets NNT=62 NNT=57 NNT=18 Well tolerated after ~10,000pts excluded!
IDEALJAMA,Nov 2005 n=8888 4.8yr • Intensive lipid lowering in previous MI pts (open label trial) • LDL: 3.14 baseline mmol/L 2.1atorv80mg vs 2.7 simv 20-40mg;Age<80, ~62 • 1o Primary: Coronary Death, nonfatal MI or cardiac resusc.9.3 vs 10.4% NS • 2o Major vascular events (1o & stroke) NNT=59/4.8yr;MI6 vs 7.2% NNT=84 • LFT's NNH=112; All-cause death8.2 vs 8.4% or CV death5 vs4.9 butat least non-CV death 3.2 vs 3.5 NS Atorvastatin 80mg/d $87 vs Simv 20-40mg/day $41 % patients NNT=59 / 4.8yr (RRR=13%) NNT=NS NNT=NS LFTs 3xNNH=112 -not powered to detect NOdifferenceinprimary endpoint orall-causedeath;CV+strokeevents; ADRs causing discontinuation
ASCOTLancet,April 2003 n=10,305 • Evidence for:primary prevention of CHD and stroke in highrisk, • middle aged, hypertensive, male patients with TC <6.5mmol/L • Questions remaining: women n=1942; adverse & long term effects; • safety and efficacy of titrating dose to attain targets & magnitude/$ 1o Prevention in high risk (Average 3.7 risk factors in addition to HTN) (HTN,male/female,age~63 40-79,TC<6.5mmol/L) Atorvastatin 10mg/d over average 3.3yrs NNT=NS NNT=91 NNT=143 Older males with multiple risk factors benefit.
TNTNEJM,April 2005 n=10,001 4.9yr • Intensive lipid lowering in stable CHD (n=15,464 - 8wk run-in) • LDL: 3.9 baseline mmol/L 2.0atorv80mg vs 2.6 atorv 10mg;Age 35-75, ~61 • 1oend point: “CHD Death, CV Event or Procedure, Stroke” • CV & Stroke events; NNT=46 / 4.9yr; • LFT's NNH=100; All-cause death5.7 vs 5.6% BUT non-CV death 3.2 vs 2.5 NS Atorvastatin 80mg/d $87 vs 10mg/day $67 % patients NNT=26 / 4.9yr (RRR=20%) NNH=NS LFTs 3xNNH=100 CV events; ADRs; NO difference in all-cause death
For patients with low HDL, high TG, but low LDL (e.g. common in diabetes) NO evidence yet for mortality benefit ADRs: Dyspepsia/abdom pain; gallstones, myopathy Differences: Evidence? Potency? Cost? Fibrates 2 Prevention Gemfibrozil 600mg/bid 1 Prevention Gemfibrozil 600mg/bid % patinets NS NNT=14 NS NNT=28
FIELD StudyIs a fibrate useful in Type 2 DM? Not really • 9795 patients age 50-75 with Type 2-DM; RCT • Fenofibrate 200mg OD vs Placebo (~5yr) • No in coronary events 1 Endpoint; did CV events. {Meta-analysis: in all-cause mortality with fibrates(NNH=132 over 4.4yrs)Studer 2005 Arch Int Med; FIELDconsistent.} NNT=NS NNT=69 NNH=NS Lancet 2005;366:1849-61.
Newsletters, Links, Email Updates... www.RxFiles.ca It’s all in the detail!
Risks from lipid lowering?Rhabdomyloysis NNH=10 RR 5.4x NNH=1,670 NNH =22,700 1) Graham DJ, et al. Incidence of hospitalized rhabdomyolysis in patients treated with lipid-lowering drugs. JAMA. Dec 2004 (24 cases of rhabdo / 252,000 pts) 2) Bandolier: Rhabdomyloysis with statins Jan 2005;131-2. http://www.jr2.ox.ac.uk/bandolier/