Download
1 / 23
230 likes | 452 Views
Procedures. Intermediate Format Cleft Lip and Cleft Palate (Cheiloschisis and Palatoschisis). Objectives. Assess the related terminology and pathophysiology of the ________________. Analyze the diagnostic interventions for a patient undergoing a cleft lip or cleft palate repair.

E N D
Procedures Intermediate Format Cleft Lip and Cleft Palate (Cheiloschisis and Palatoschisis)
Objectives • Assess the related terminology and pathophysiology of the ________________. • Analyze the diagnostic interventions for a patient undergoing a cleft lip or cleft palate repair. • Plan the intraoperative course for a patient undergoing_____________. • Assemble supplies, equipment, and instrumentation needed for the procedure.
Objectives • Choose the appropriate patient position • Identify the incision used for the procedure • Analyze the procedural steps for_____________. • Describe the care of the specimen
Terms and Definitions • Cleft: split or gap between two structures that are normally joined
Definition/Purpose of Procedure • Cleft Lip Goal: symmetry of nostril floor and nostril sil and a natural appearance of cupid’s bow • Strive for functional repair of muscles with an aesthetically pleasing approximation of the skin edges; resolve sucking difficulties • Palatoplasty: to form the absent roof of the mouth; prevent the escape of air thr the nose during speech, keep food and fluids out of the nose, and facilitate sucking and eating
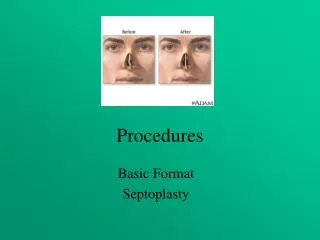
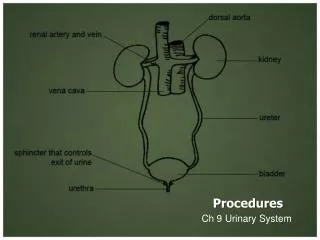
Pathophysiology Unilateral cleft lip Unilateral cleft palate
Surgical Intervention:Special Considerations • Patient Factors • Increase room temperature or apply webril to limbs for warmth, depending on age; cap for head • Family communications hourly • Room Set-up—ESU, Suction, lights, radiant heat lamp over OR bed until pt in room; may increase room temp to 80 degrees F (26.7 C)
Surgical Intervention: Positioning • Position during procedure • Supine w/head at very top of bed • Bed will be turned 90 degrees after induction—be sure to turn bed around to allow “knee room” for surgeon while sitting • Supplies and equipment • Gel padding • Shoulder roll for increased palatal exposure • Special considerations: high risk areas
Surgical Intervention: Special Considerations/Incision • Special considerations • Surgeon inserts cleft palate mouth gag and infiltrates palatal structures with 5 mg/kg of 0.25% lidocaine w/epi 1:400,000 using a 3 mL syringe (resulting in hydrodissection of palatal structures, decreasing intrap bleeding) • Neonate’s face is prepped with Betadine solution x 3, to include the mouth gag and mouth, and avoiding pooling of solutions • State/Describe incision
Surgical Intervention: Supplies • General • Specific • Suture: 5-0 Braided absorbable; 7-0 Chromic • Blades: # 15 • Medications on field (name & purpose) • 0.25% lidocaine w/epi 1: 400,000 • Surgical Glue • Catheters & Drains • Plastic Surgery Specialty Cart
Surgical Intervention: Instruments • General: Plastic surgery “local” instrument set; oral instrumentation set • Specific • Brown lip clamps, calipers, a Fomen retractor, Beaver Blades # 64 and # 65, Logan bow, Dingman mouth gag and assorted retractor blades • (Palate) Blair palate hook, palate knives, Blair palate elevators, Fomen lower lateral scissors, short & long
Surgical Intervention: Equipment • General • Specific • Radiant warmer for bed preop
Surgical Intervention: Procedure Steps • Normal landmarks are identified and marked or tattooed. • Calipers & a ruler are used to make precise measurements so that corresponding points are marked along the cleft. • Surgeon places raytex sponge in back of neonate’s throat to minimize the amt of blood ingested & makes incision along hard palate. • Surgeon exposes the tensor veli palatini & levator palatini muscles, but only as much as needed to limit scarring. • * scarring increases risk for palate immobility post-op • Surgeon makes releasing incisions along the lateral aspects of the soft palate so there is no tension along the median closure line.
Surgical Intervention: Procedure Steps • Surgeon makes additional incisions in the nasal mucosa and the posterior edge of the soft palate musculature where it is abnormally attached to the hard palate • Surgeon elevates the oral mucosa just enough for edges to be sewn together. (Suture size depends on neonate size) • Beginning with the uvula and working anteriorly, the surgeon closes the mucosa on the nasal side using a 4-0, 5-0 or 6-0 braided absorbable suture w/small specially designed fishhook needle. • Surgeon closes the oral mucosa and muscle layers using braided absorbable suture in horizontal mattress fashion. • Surgeon places cellulose gauze over raw surfaces of the hard palate to assist with hemostasis (dissolves in 7-10 days).
Surgical Intervention: Procedure Steps • Surgeon places a traction suture in the neonate’s tongue, which can be used if postop airway obstruction occurs • Mouth gag is carefully removed, being careful to avoid extubation. • Cleft Lip repair begins when the surgeon tattoos the desired anatomical design of the lip with MB, then injects 0.25 % lidocaine w/epi 1: 400.000. • 2 Techniques exist: Tennison-Randal Triangular Flap And the Millard rotational advancement technique (more common) In most procedures, 5-0 braided absorbable suture on a small cutting needle is used for closure of the muscle layer.
Surgical Intervention: Procedure Steps • Surgeon uses 7-0 chromic, followed by surgical glue, to close the skin. • No further dressing is needed— • Throat pack is removed, and the neonate is extubated.
Counts • Initial: sponges and sharps • First closing • Final closing • Sponges • Sharps
Specimen & Care • Identified as N/A • Handled: routine, etc.
Resources • STST pp. 696-697; 713-715 • Alexander’s pp. 1235-1237 • Boegli, Rogers, & McGuinness Complete Review of ST • AORN Journal Mar 2002 “Repairing Cleft Lip and Palate Deformities” pp. 490-499 by Sandberg, Magee, & Denk