Download
1 / 13
160 likes | 405 Views
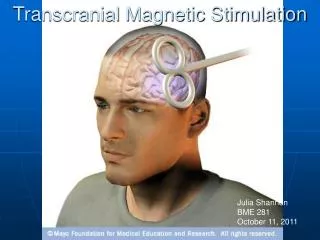
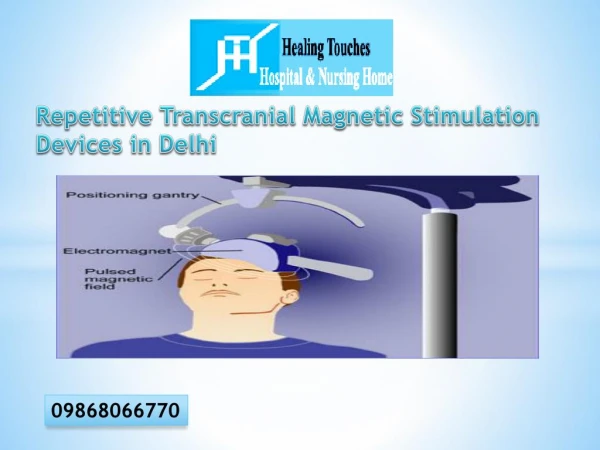
Transcranial Magnetic Stimulation (TMS). Rapid magnetic field changes >> electric current Magnetic field created at scalp with figure-8 coil Electric current induced in neurons in cortex Adds noise, disrupts coordinated activity Temporary “lesion”

E N D
Transcranial Magnetic Stimulation (TMS) • Rapid magnetic field changes >> electric current • Magnetic field created at scalp with figure-8 coil • Electric current induced in neurons in cortex • Adds noise, disrupts coordinated activity • Temporary “lesion” • Without the kind of compensation that develops w/ long-term lesions • Apply to different areas of scalp & see what functions disrupted • Disruption does NOT mean brain regions directly under coil responsible for function • Only that it’s involved somehow in the function • OR connected to regions involved in the function • Get distal effects through connections (“diaschisis”)
TMS Coil Naeser et al. (2004), Fig 2, p 100 Maximum magnetic field at center of figure-8
Rapid-onset brief electrical current generated in coil Produces rapid-onset brief magnetic field pulse (up to 2 Tesla) Induces rapid-onset brief electrical field Induces rapid-onset brief electrical current in brain (mostly cortex) Which has an effect on some task Walsh & Cowey (2000), Fig 2, p 76
Repetitive TMS (rTMS) • Most studies so far have used rapidly repeated trains of magnetic pulses • Because single pulses weren’t found to have much effect on gross measures of behavior early on • But more recently, single pulse studies have found effects when have constrained hypotheses & more sensitive behavioral measures • Can time single pulse at different steps in a process to see when it has the most effect • Very little so far • Mostly studying vision & motor processes
TMS & Language • Stewart et al. (2001) Stewart, Walsh, Frith, & Rothwell (2001), Neuroimage, 13, 472-478. • rTMS during speech • Monitored speech, EMG, & videotaped • rTMS at a more posterior frontal region of both the LH & RH produced both • Speech arrest • & EMG in mentalis muscle • At a more anterior frontal region, only LH stimulation produced • Speech arrest • But no EMG in mentalis • So, probably different causes of the 2 kinds of speech arrest, & only LH stim leads to the non-muscular type
More TMS & Language • Knecht et al. (2002) Knecht, Floel, Drager, Breitenstein, Sommer, Henningsen, Ringelstein, & Pascual-Leone (2002), Nature Neuroscience, 5, 695-699. • Goal: Evaluate the functional significance of varying degrees of language lateralization • Evaluated lateralization in large sample during silent word production task w/ • Functional transcranial Doppler sonography (fTCD) • fMRI • Grouped subjects into 5 categories from very strongly left lateralized to very strongly right lateralized • Many more subjects w/ L than w/ R lat • Task: Picture-word verification
Knecht et al. cont’d • rTMS applied during task to • L & R language areas (CP5 & CP6, ~ Wernicke’s area) • Midline occipital region (Oz) • Control, not expected to affect task performance • 1 Hz for 10 min*, w/ 30 min* rest between trains • Produces disruption lasting up to several minutes • Significant correlation between degree of slowdown & inaccuracy in task w/ degree of lateralization • More strongly L-lateralized, more disruption w/ LH stim • More strongly R-lateralized, more disruption w/ RH stim • Less lateralized, less disruption w/ either H stim * Notice corrections since in-class presentation
TMS vs Wada Test • Neurosurgeons routinely use pre-surgical Wada Test to determine gross lateralization of language • So can spare language-related tissue • Risky – occasionally causes stroke • TMS less risky, & some proponents argue it should replace Wada test • But others argue that Wada & TMS on the same person disagree too often to rely on TMS yet
TMS as Therapeutic Tool • Already used in treatment of depression • Naeser et al. (2004) Naeser, Martin, Nicholas, Baker, Seekins, Kobayashi, Theoret, Fregni, Maria-Tormos, Kurland, Doron, & Pascual-Leone (2004), Brain & Language, 93, 95-105. • Functional imaging studies on non-fluent aphasics often show more activation in RH homologues of LH language areas than normals do • Does this represent some kind of adaptive strategy? • Is it actually maladaptive? • Could TMS suppress this activity, & lead to better language??
Naeser et al. cont’d 4 non-fluent patients, 5-11 years post-stroke Naeser et al. (2004), Fig 1, p 99; (Radiological convention = L & R reversed)
Naeser et al. cont’d • rTMS over RH homologue of Broca’s area • Daily for 10 days, 20 min each time • Tested picture naming speed & accuracy • Immediately after 10th session • All patients reliably faster & more accurate than their pre-treatment baseline measures • 2 months later & 8 months later • Effects decreased over time, but continued through 8 mos for 3 of 4 patients
The Right Hemisphere (RH) & Language • The RH • Retrieves & holds onto infrequent & contextually inappropriate meanings of ambiguous words • Long after the LH settles on what seems to be the contextually appropriate meaning • Plays critical role in understanding non-literal language • Puns, idioms, metaphors, sarcasm, etc. • Maybe it’s the RH’s job to hold onto stuff that might be relevant, just in case things don’t turn out as the LH thought they would • LH’s job to make quick decisions, which means it’s sometimes going to be wrong & need what RH has kept
TMS Study I’d Like to See • What would happen if apply TMS to RH during the comprehension of ambiguous words or idioms or sarcasm? • How much would effects depend on timing of pulse(s)? • How would pulse(s) earlier vs later during the processing of ambiguous words influence whether get priming for targets related to contextually irrelevant meanings of ambiguous words? • How would pulse(s) earlier vs later during idiom comprehension influence whether you get the idiom? • …