Download
1 / 25
290 likes | 1.81k Views
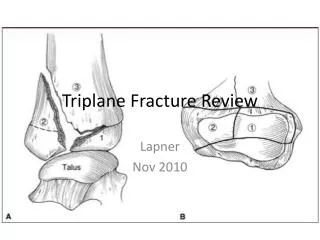
The Pediatric Triplane Ankle Fracture. Mitchell Goldflies, M.D. Overview. Introduction History Pathophysiology Diagnosis Treatment Closed Open Discussion. Pediatric Triplane Ankle Fracture. Complex fracture Difficult to define according to Salter-Harris classification.

E N D
The Pediatric Triplane Ankle Fracture Mitchell Goldflies, M.D.
Overview • Introduction • History • Pathophysiology • Diagnosis • Treatment • Closed • Open • Discussion
Pediatric Triplane Ankle Fracture • Complex fracture • Difficult to define according to Salter-Harris classification
Pediatric Triplane Ankle Fracture con’t • Meets three-plane criterion • Represents 5 – 10% of pediatric intra-articular ankle injuries • Presents in children age 12 to 15 years of age • Higher incidence among boys • Treatment: • Nondisplaced triplane/extra-articular injuries: • Immobilization in long leg cast • Displaced: • Open reduction and internal fixation
History • Lynn • 1972 • Termed injury pattern distal tibial epiphyseal • Produced by combination of mechanisms and characteristic asymmetric pattern of closure
History con’t • Marmor • Three fragments requiring cortical screw fixation found
Pathophysiology • Susceptible during transitioning skeletal maturity: • Girls:12 to 14 years of age • Boys:13 to 15 years of age • Not younger then age 10 or older than 16.7 years
Pathophysiologycon’t • Sustain injury during athletic activity or consequence of fall • Increased incidence among skateboarding, roller skating, inline skating, ice skating, and snowboarding
Pathophysiology con’t • Three fracture fragments: • Fracture fragments mimic the juvenile Tillaux fracture • posterior and medial fragments with a metaphyseal spike, and the tibial metaphysis • Fibular fracture in approximately 50% of triplane ankle fractures
Pathophysiology con’t • Two fracture fragments: • Lateral: • coronal fragment posterolateral • Medial: • coronal fragment posteromedial • intra- and extra-articular intramalleolar variants have been described
Pathophysiology con’t • Quadruple fracture fragments: • External rotation and vertical compression proposed as mechanism for injury
Diagnosis • Radiographs • Do not consistently demonstrate the number of fracture fragments • Anterposterior radiographs: • triplane fracture has appearance of Salter-Harris type III • Lateral radiographs: • triplane fracture has appearance of Salter-Harris type II
Diagnosis con’t • CT Scans • Used to: • identify configuration of the facture • aid in evaluating residual displacement, • aid in preoperative planning • Three-point star configuration noted
Diagnosiscon’t • MRI • Used for: • complex fractures • fractures of uncertain classification based on radiographs
Diagnosis con’t • Brown et al study • 51 children aged 10 to 17 years • Most frequent: two-fragment pattern with medial epiphyseal extension (33/51 children) • Three-fragment patterns seen • Extension to medial malleolus evident (12 children)
Treatment • Selection based on: • Fracture is nondisplaced or displaced • Magnitude of displacement • Intra- versus extra-articular nature of injury • Fractures with >2mm intra-articular step-off require reduction (closed or open)
Treatment – Closed • Nondisplaced triplane and extra-articular fractures (<2mm displacement): • Managed with long leg cast • Closed reduction performed under general anesthesia with axial traction on the ankle and internal rotation of the foot • Reduce fibular fracture first • Medial fractures: • external rotation foot position • Lateral fractures: • internal rotation foot position
Treatment – Closed con’t • Nondisplaced triplane and extra-articular fractures (>2 mm displacement): • Requires open or closed reduction • Nondisplaced triplane and extra-articular fractures (>3 mm displacement): • Closed reduction not successful • Extra-articular variants • Nonsurgical management
Treatment - Open • ORIF • Anterolateral approach – lateral fractures • Anteromedial approach – medial fractures • Surgical indications: • Fracture displacement >3 mm • Failure to achieve adequate reduction (>2 mm intra-articular step off)
Treatment – Open con’t • Arthroscopic reduction and internal fixation of two-part triplane fractures • Advantages: • surgical trauma reduced • clearer identification of fracture fragment orientation • allows for direct visualization of joint congruity and accurate reduction
Discussion • Distal tibial physis • 50% of tibial growth • 4 to 6 mm of longitudinal growth per year • Surgical treatment as measure to prevent residual articular incongruity and long-term degeneration • Most patients return to preinjury activity levels
Conclusion • Unique fracture configuration • Not consistent with Salter-Harris classification • Results from asymmetric closures of distal tibial physis and combination of mechanisms • Proper diagnosis and treatment requires: • Evaluation/awareness of associated injury • Understanding of fracture patterns possible • Radiographs and CT necessary to evaluation conduct preoperative planning • Rational treatment approach • Optimal treatment: • Reduction to within 2mm of anatomic
Resources • Journal of the AAOS. Vol. 15. No. 12. pp. 738 – 745.