Download
1 / 14
140 likes | 458 Views
Cardiac Assessment and Diagnostic Procedures. NPN 200 Medical Surgical 1. Assessment. Subjective Interview Why did you seek medical attention? What symptoms are you having? Weight gain, dyspnea, fatigue, cough, palpitations, chest pain (describe), syncope, dark urine, edema

E N D
Cardiac Assessment and Diagnostic Procedures NPN 200 Medical Surgical 1
Assessment • Subjective Interview • Why did you seek medical attention? • What symptoms are you having? • Weight gain, dyspnea, fatigue, cough, palpitations, chest pain (describe), syncope, dark urine, edema • Previous medical history • Any family history of ^ B/P, heart disease, diabetes? • How has this illness affected your lifestyle? • Smoking history, diet, physical activity
Assessment • Physical or objective • Height, weight • Heart sounds • Aortic, pulmonic, tricuspid, and mitral • Listen for extra sounds , S3 and S4 • Murmurs, rubs (best heard over the left sternal border) • Vital signs • B/P lying, sitting and standing • apical and radial pulse with the quality according to scale of 0-4 • Respirations, effort and skin color, with breath sounds
Assessment, cont • Skin • Color • Hair distribution • Capillary refill • Extremities • Inspect and palpate for: • Color • Edema- 1+, 2+, 3+, 4+ • Warmth- lowered in heart failure, PVD, and shock • Pulse quality- strong, weak, thready • Clubbing
Venous and Arterial Pulses • Check Jugular vein distention • Must assess all major peripheral pulses • Will indicate hypovolemia, decreased cardiac output • Must check for symmetry • Can auscultate the carotid, and the aorta
Diagnostic Procedures • Electrocardiogram (ECG) • Studies the conduction system • Electrodes placed on the skin pick up the electric impulses • Placement of pads determines the area of the hearts electrical activity • The cardiac cycle is represented by a wave ( P,Q,R,S )
Diagnostic Procedures, cont. • Holter monitor • Echocardiogram • Transesophageal Echocardiogram • MRI • MUGA (multiple-gated acquisition scan) • Stress Test • Cardiac Cath • EPS (electrophysiology study)
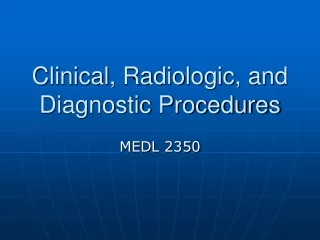
CARDIAC CATH • Prep for Cardiac Cath • May be done as and outpatient • Chest x-ray, EKG, CBC, coagulation studies • NPO or light breakfast • Shave, & cleanse • Check for allergies • Total assessment • Teach client • Mild sedative may be given • Post care- lie flat, bedrest, may use a closure device, vital signs, CMS, cath site
Diagnostic Procedures, cont • Laboratory Tests • ABG’s • Pulse oximetry • Cardiac enzymes or CPK isoenzymes • CPK (creatinine phosphokinase) – found in high concentrations in skeletal, brain and heart muscle • CPK-MB – found in heart tissue, rises in 4-6 hours after damage to heart muscle, and peaks in 12-24 hours at more than 6 x the normal value, then returns to normal in 2-3 days
Diagnostic Procedures, cont • Cardiac enzymes • LDH (lactate dehydrogenase) • High concentrations in the heart, skeletal, and brain tissue. • Used as an indicator of damage to heart muscle, along with other labs
Complete Blood Count (CBC) • WBC is used to determine if there is inflammation or infection (AMI leads to inflammation and endocarditis is infection) • RBC’s,HGB & HCT indicates the O2 carrying ability of the blood • Platelets are necessary for coagulation and the count may be increased in some acute infections and heart disease • Myoglobin released soon after cardiac muscle damage • 1-4 hrs after symptoms • May also be elevated in skeletal muscle • Troponin is a protein and is used in muscle contraction • 2 subtypes are found in the blood after an MI • Levels rise in 3-6 hours after symptoms, peak in 24 hrs and may be found up to 2 wks • Results available quickly (15 to 20 min) in the ER
Lipid Profile • Composed of : Cholesterol, triglycerides, serum lipids, and phospholipids • Considered a risk factor for CVD • ^ B/P, and MI • Cholesterol may be non-fasting • Produced by the liver • CAD risk ^ 3x if greater than 260 • Must work to keep below 200 • HDL and LDL • Triglycerides need to be drawn after 12 hrs fasting