Download
1 / 21
240 likes | 810 Views
Cardiac Assessment 2. Alison Ketchell HECS 2063. Brief cardiac physiology revision Cardiac failure Assessment in practice 2 ~ ‘The breathless patient’. Cardiac anatomy. Pulmonary arteries Pulmonary veins Left atrium Mitral (bicuspid) valve Aortic valve

E N D
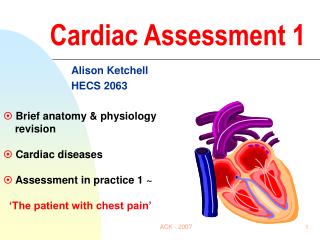
Cardiac Assessment 2 Alison Ketchell HECS 2063 • Brief cardiac physiology revision • Cardiac failure • Assessment in practice 2 ~ ‘The breathless patient’ ACK - 2007
Cardiac anatomy Pulmonary arteries Pulmonary veins Left atrium Mitral (bicuspid) valve Aortic valve Left ventricle Septum Endocardium Myocardium Pericardium Aorta SVC Right atrium IVC Tricuspid valve Pulmonary valve Right ventricle ACK - 2007
Cardiac physiology • CARDIAC OUTPUT ~ the volume of blood ejected by either ventricle per minute COdetermined byHR X SV • HEART RATE (HR) = Number of beats per min • STROKE VOLUME (SV) = Volume of blood ejected during systole from each ventricle per beat • Average cardiac output of adult at rest = 75 x 70 = 5.25 litres / minute per ventricle ie entire circulatory volume • BLOOD PRESSURE (BP) ~ the pressure of blood exerted against the vessel wall BP determined by CO X PVR ACK - 2007
Causes of cardiac failure • Reduced contractility caused by:- ~ Acute coronary syndrome (ACS) ~ Cardiomyopathy ~ Infection, hypoxia, alcohol, acidosis • Volume / pressure overload:- ~ Valve disease • Insufficient volume caused by:- ~ Hypovolaemia ~ Constrictive pericarditis, valve disease • Precipitating factors:- ~ Electrical disorders, drugs, infection Left ventricular failure and / or congestive cardiac failure ACK - 2007
Cardiac failure • A state in which CO is insufficient to meet metabolic needs of the body • Inadequate cardiac performance leads to:- • Congestion of tissues or organs - LV : LA dysfunction pulmonary venous congestion - RV : RA dysfunction systemic venous congestion • Insufficient perfusion of tissues or organs - Low BP (despite adequate PVR) - Usually referred to as acute circulatory shock or cardiogenic shock • Cardiac failure = clinical manifestation of signs & symptoms associated with inadequate cardiac performance ACK - 2007
Compensatory mechanisms triggered to maintain CO CO = BP ~ reflex ST 1) LV dilatation Starlings Law LV hypertrophy 2) SNS stimulation = HR 3) Renal blood flow = Renin release Angiotensin I Angiotensin converting enzyme (ACE) Angiotensin II Vasoconstriction ++ 4) Aldosterone release = NA+ retention (H20) 5) Arginine vasopressin (ADH) release = Water retention 6) ANP : BNP release ACK - 2007
Effect Circulating volume vasoconstriction 1) preload & afterload 2) Cardiac workload DECOMPENSATION ~ excess cardiac / extra cardiac compensation clinical manifestation 3) LVEDP & LAP 4) Pulmonary artery pressure (PAP) 5) Systemic venous pressure ACK - 2007
Clinical signs ~ left ventricular failure (LVF) Pulmonary artery pressure (PAP) Pulmonary oedema 1) SOBE ++ 2) SOB @ rest 3) Reduced O2 saturation 4) Orthopnoea 5) Paroxysmal nocturnal dyspnoea (PND) 6) Frothy sputum 7) Cyanosis ACK - 2007
Clinical signs ~ (Congestive) cardiac failure Systemic / central venous pressure Peripheral oedema 1) Raised JVP / CVP 2) Gravitational pitting oedema : ascites 3) Hepatomegaly : jaundice 4) Splenomegaly 5) Proteinurea 6) Anorexia : constipation : cachexia 7) Mental tirdeness : fatigue : confusion : low GCS ACK - 2007
Mr X complains of acute breathlessness • Emergency / acute phase ~ 1st hour • ABC assessment priority …. then glean more detail • Establish presentingcomplaint ~signs / symptoms • Relief of symptoms • Haemodynamic status • Differential diagnosis • Initiate prompt treatment • BLS / ALS available ACK - 2007
Establish presenting complaint ~ signs & symptoms Patient history ~ breathlessness - Respiratory rate - Effort - Noise - Exertional dyspnoea - Orthopnoea - Paroxysmal nocturnal dyspnoea - Cough - Sputum ACK - 2007
Associated signs & symptoms - Pain - Nausea / vomiting - Sweating, pale, cold, clammy - Restless - Palpitations - Syncope - Oedema - Cyanosis ACK - 2007
Relief of symptoms • Breathlessness ~ - Bed rest - High flow O2 therapy via non re-breathe bag - 10 – 15L/min (95 – 98%) NB COPD !! - IV Diamorphine 2.5 – 5mg - IV Frusemide 80mg • Anxiety ~ - Simple, repetitive information - Visibility, approachability ACK - 2007
Haemodynamic status • General – skin colour, warmth, ? distressed, temperature, posture, accessory muscle • Pulse - rate, regularity & rhythm – cardiac monitor • BP & fluid balance • Respiration - rate, depth, O2 saturations, ABG’s, sputum • 12 lead ECG • Venous blood sampling – FBC, U&E’s, TFT’s, LFT’s, Cholesterol, Troponin, CK / CKMB, CRP, Cultures? Clotting? ACK - 2007
Other immediate investigations - JVP, precordial palpation, chest auscultation • CXR - interstitial : alveolar oedema : cardiomegaly pleural • effusion, ABG’s - Echo ~ TTE or TOE - Urinary catheter • - Drug history - Systemic enquiry - ?? Invasive haemodynamic pressure monitoring – Swan ganz ACK - 2007
New York Heart Association classification (NYHA) • I No symptoms at rest, dyspnoea on vigorous exertion • II No symptoms at rest, dyspnoea only on moderate exertion • III May be mild symptoms at rest, dyspnoea on mild exertion, severe dyspnoea on moderate exertion • IV Significant dyspnoea at rest, severe dyspnoea on mild exertion or bed bound ACK - 2007
Initiate prompt treatment - acute pulmonary oedema • Treat cause – revascularise, replace valve, restore SR • Treat fluid / volume overload - IV Frusemide 80mg + thiazide - Fluid balance record • Treat reduced CO & perfusion - Bed rest - ACEI or antagonists - IV Nitrate - IV Inotropes • Impaired gaseous exchange - 8 – 10L/min O2 ACK - 2007
Initiate prompt treatment - acute pulmonary oedema • Ineffective breathing pattern - IV Diamorphine 2.5mg - NIPPV / CPAP • Oral aspirin (75 – 150mg daily) • SC LMWH - Clexane • Oral statin • Reduced exercise tolerance • Knowledge deficit • Anxiety & fear • Feelings of hopelessness & loss of control • Next of kin ACK - 2007
The next 12 hours • Bed rest & continuous monitor & O2 sats on CCU / cardiology • Full biographical & nursing assessment – ADL’s • Further history - Past medical history (PMH) • - Social history (SH) & family history (FH) • - Risk factors (RF’s) • - Drug history (prescribed & social) ACK - 2007
Ongoing care • Observe - 4 hourly Temp, P, BP, R, O2 sats • - Fluid balance chart, urinalysis, ?? BM stix • - ?? Daily weight • Bed rest complications - C/o ventilation therapy - Pressure area care, mobility - Hygiene & toilet needs - Diet & fluids - C/o IV access, urinary catheter - Psychological & social support ACK - 2007
Pre ….. Post discharge • Other specific investigations & intervention • - ? Modified ETT, Dobutamine stress test, CT scan, MRI • - ? Angiography …… PTCA ….. stent …. CABG • - ? DC cardioversion • Cardiac rehabilitation - Heart failure specialist nurse - Return to ‘normal’ healthy lifestyle - Information, advise, counselling - Medication - Smoking cessation - Diet - Exercise - Anxiety ACK - 2007