Download
1 / 94
1.11k likes | 1.35k Views
Respiratory System Anatomy. Fig. 22.1. Upper respiratory tract Vs. Lower respiratory tract Conducting Zone Vs. Respiratory Zone. Conducting Zone Passages no exchange. Fig. 22.7. The Bronchial Tree no exchange. Fig. 22.11. Respiratory Zone Structures gas exchange. Fig. 22.8.

E N D
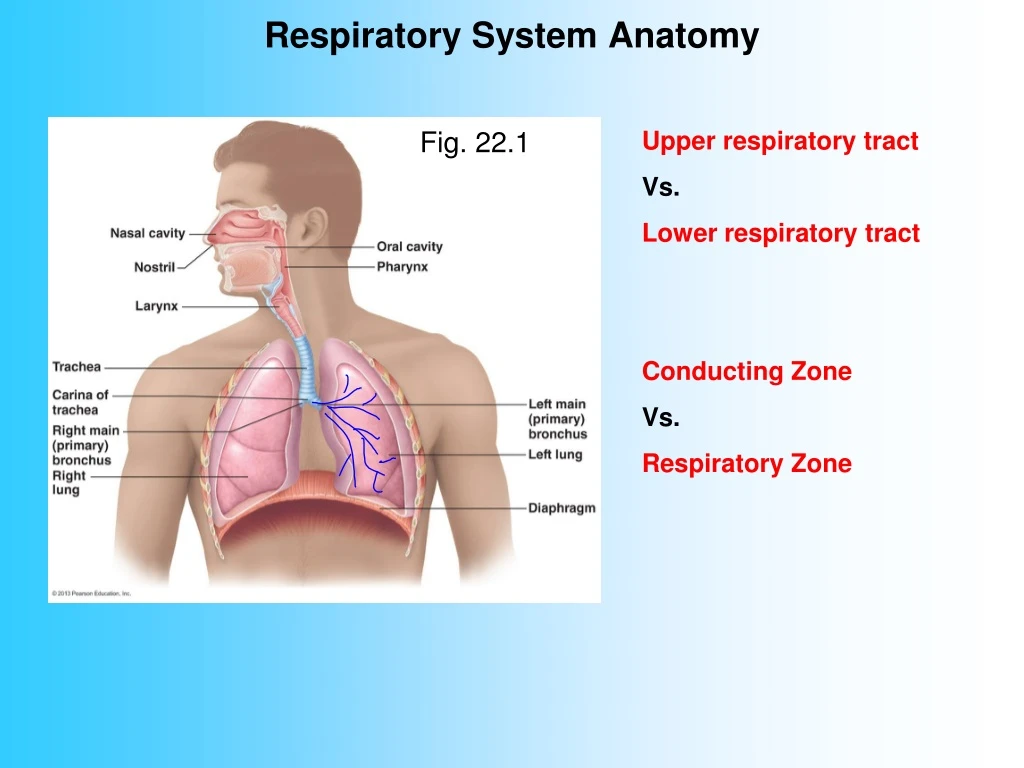
Respiratory System Anatomy Fig. 22.1 Upper respiratory tract Vs. Lower respiratory tract Conducting Zone Vs. Respiratory Zone
Conducting Zone Passagesno exchange Fig. 22.7
The Bronchial Treeno exchange Fig. 22.11
Respiratory Zone Structuresgas exchange Fig. 22.8
Alveoli & The “Respiratory Membrane” Fig. 22.9
Alveoli & The “Respiratory Membrane” Fig. 22.9
Alveoli & The “Respiratory Membrane” Fig. 22.9
Relevant Pressures Atmospheric… Intrapulmonary (alveolar)… Intrapleural… Fig. 22.12
Intrapleural pressure is always negative. Why? • Ans: Lung Recoil • Due to: • Elasticity • 2. Surface Tension • inside alveoli a.k.a. alveolar
Surface tension inside alveoli Fig. 22.9 Video: Surface tension of water
So why don’t your lungs collapse?a.k.a. “Would you like to win $20?” They recoil but they don’t collapse Why? Ans: Surface Tension Between the pleural membranes (Not inside the alveoli) Fig. 22.12
Pulmonary Ventilation • Definition… • Air only flows when… • Gradient is bt atmospheric and intrapulmonarynot intrapleural • Boyle’s Law says… • So, to cause ventilation we must… Fig. 22.12
Inspiration vs. Expiration “active” “passive” Fig. 22.1
Lung Compliance • Definition… • Increased 10X by surfactant • Decreased by: • lack of surfactant • Fibrosis • Restricted airways • reduced flexibility of rib cage Fig. 22.1
Clinical Application Atelectasis…
Clinical Application Pneumothorax…
Clinical Application Hemothorax… Hemopneumothorax…
Clinical Application Trtmt: Chest tubes
Clinical Application Tension Pneumothorax… Trtmt: “needle decompression”
Clinical Applications • IRDS • Common in… • Premature births • C-section births • 3 components: • Lack of Surfactant • Small, non-compliant alveoli • Weak chest wall muscles Trtmt…Pos. Pressure ventilation + surfactant Days 1-3 critical…
Dalton’s Law of Partial Pressuresa.k.a. “the PP lecture” Says… E.g. Ambient air in this room is a mixture of: N2, O2 & C02 Atmospheric pressure = 760 mm Hg Each gas contributes a ‘part’ of the total pressure [O2] = 21% 760 mm Hg X 0.21 = 160 mm Hg Partial pressure of O2 = 160 mm Hg PO2 = 160 mm Hg [CO2] = 0.04% 760 mm Hg X 0.0004 = 0.3 mm Hg Partial pressure of CO2 = 0.3 mm Hg PCO2 = 0.3 mm Hg
Fig. 22.17 But alveolar PPs are not same as atmospheric PPs PO2 is 104 not 160 mm Hg PCO2 is 40 not 0.3 mm Hg Why? Tidal volume (500 ml) mixes with residual volume (2400 ml)
Henry’s Law Video overview… 3 min Henry’s Law says… Assumption: the gas is soluble in the liquid • CO2 is most soluble • O2 is soluble but 20X less than C02 • N2 is nearly insoluble Fig. 22.9 • Blood ‘picks up’ the PP values of alveolar air, not ambient air • **Gas quality of the blood will never be any better than…
Gas Exchange External Respiration Vs. Internal Respiration Driven by PP Gradients Fig. 22.17
External Respiration occurs at the respiratory membrane Fig. 22.9 alveolar air blood
The Respiratory Membrane Fig. 22.9 • Consists of: • Two thin cells • Connective tissue and ISF betweencells • Fluid lining insides of alveoli • Massive… covers1300 s.f. (in HS103…= floor & both side walls) • May be thickened by: pneumonia, lung cancer (CA), tuberculosis (TB), cystic fibrosis (CF), etc. • May be eliminatedbyemphysema
Ventilation-Perfusion Coupling(similar to local reg. of BF…) Fig. 22.19
AAAGGGHhhhhhhhhhhhhhhhhhhhhhhh! Fig 22.22
Want to turn your AAGGHhhh! into oooOOOOOooooo ? O2 CO2 Hb HbO2 HHb HbCO2 H+ HCO3- H2CO3 CO HbCO Oxygen Carbon dioxide Hemoglobin Oxyhemoglobin Deoxyhemoglobin Carbaminohemoglobin Hydrogen ion Bicarbonate ion (a.k.a. Bicarb) Carbonic acid Carbon monoxide Carboxyhemoglobin
External Respiration at the lungs… Fig 22.22
Internal Respiration at the tissues… Fig 22.22
Gas Transport • O2 • O2
Gas Transport • CO2 • CO2 • CO2
Factors Decreasing Affinity of Hb for 02 Change Effect on Effect on At Tissue Affinity ease of release • PO2 • PCO2 • Temp • pH
Cyanosis – Special Case • S&S • 47y.o. male • One month arthralgia • 2 days fever, arthralgia, N&V, & diarrhea • Cyanosis of extremities • Death
Cyanosis – Special Case • Autopsy… • Multiple microaneurysms • Diagnosis: polyarteritis nodosa • An autoimmune disorder that damages blood vessels. • Ischemia leads to necrosis.
Clinical Application: Carbon monoxide poisoning (CO) Fig 17.4
Clinical Application: Carbon monoxide poisoning (CO) • CO competes with O2 for same binding site • Hb affinity for CO is 240X greater • Tissues hypoxic but not ischemic • Skin red • ↓ LOC… syncope • Death • Trtmt: • Remove from source of CO • Give 100% O2 • Hyperbaric chamber Fig 17.4
Q&A H2CO3 • HbCO2 HHb HCO3- CO HbO2 Hb HbCO Hb + CO2 CO2 + H20 H+ + HCO3-
The Respiratory Control Centers Fig 22.23 VRG = ventral respiratory group A ‘pacemaker’ with autorhythmicity Influenced by… Eupnea… RR = 12-20 Hyperventilation… Hypoventilation… Apnea…
Hyperventilation Def.… ‘Compensatory’ (normal) vs. ‘Noncompensatory’ (abnormal) Examples of compensatory: 1) Exercise • [CO2] will ____ • pH will ____ • Chemoreceptors tell control centers to ____ RR and depth • As a result [CO2 ] ____ • And pH ____ 2) Aspirin overdose • Acetylsalicylic acid (ASA) • So pH would ____ toward metabolic acidosis • Chemoreceptors tell control centers to ____ RR and depth • As a result [CO2 ] ____ • and pH ____
Example of noncompensatoryhyperventilation • Most often due to emotions • Too much CO2 is “blown off” resulting in hypocapnia (a.k.a. hypocarbia) • so pH would ____ • Resulting in respiratoryalkalosis • S&S • Initially: light headedness, tingling of fingers, toes, and face • Later: palpitations of heart, muscle cramps, spasms/tetany of fingers and hands