Download
1 / 30
330 likes | 587 Views
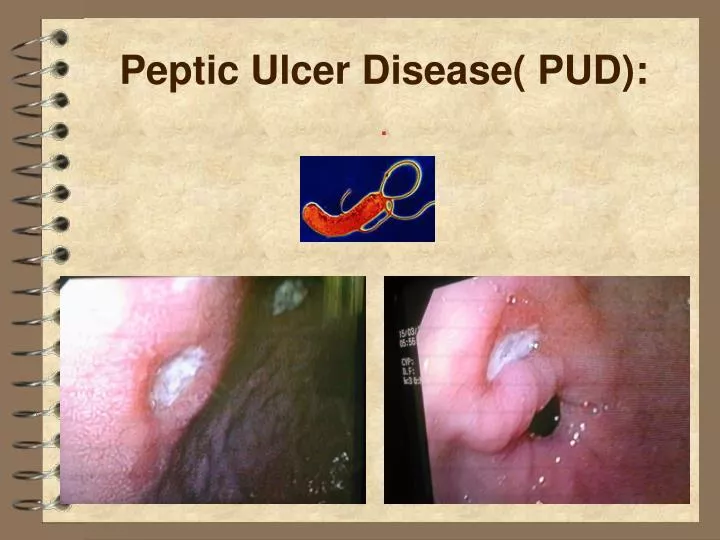
Peptic Ulcer Disease( PUD):. Introduction:. Discontinuation of the mucous membrane of the GIT. Acute or chronic; both penetrate the muscularis mucosae but in acute ulcer no evidence of fibrosis. Erosions do not penetrate the muscularis mucosae.

E N D
Introduction: • Discontinuation of the mucous membrane of the GIT. • Acute or chronic; both penetrate the muscularis mucosae but in acute ulcer no evidence of fibrosis. • Erosions do not penetrate the muscularis mucosae. • Locations: duodenum, stomach, lower oesophagus, or in the jejunum after Gastrojejunostomy or, rarely, in the ileum adjacent to a Meckel's diverticulum.
GASTRIC & DUODENAL ULCER : • The prevalence is decreasing in Western communities as a result of widespread H. pylori eradication, but high in developing countries. • Male/female for DU 5:1-2:1, for GU is 2:1 or less.
Aetiology: • H Pylori. • NSAIDs. • Smoking. • Genetics.
Aetiology: H pylori • The most important cause. • HP prevalence rises with age, 50% > 50 years are infected. • In developing world HP is much more common, usually acquired in childhood & up to 90% of the adults are infected. • The vast majority of colonised people remain healthy/ asymptomatic& only a minority develop clinical disease. • 90% DU, 70% GU are infected with H. pylori; the remaining 30% GU are due to NSAIDs.
H pylori: Pathophysio • H. pylori is Gram-negative, spiral with multiple flagella at one end which make it motile, allowing it to burrow& live deep beneath the mucus layer closely adherent to the epithelial surface. • It uses an adhesin molecule (BabA) to bind to the Lewis b antigen on epithelial cells,where the surface pH is close to neutral & any acidity is buffered by the organism's production of the enzyme urease.produces ammonia from urea, raises the pH around the bacterium & between its two cell membrane layers. • The bacteria spread by person-to-person contact via gastric refluxate or vomitus. • H. pylori exclusively colonises gastric-type epithelium& found in the duodenum only in association if there are patches of gastric metaplasia.
H pylori: Pathophysio • Causes chronic gastritis by provoking a local inflammatory response in the underlying epithelium, depends on numerous factors; bacterial factors as expresion of cagA / vacA genes & host factors.
H pylori: Pathophysio • Bacterial factots: • H. pylori strains expressing cagA (cagA+) are more often associated with disease than cagA- strains. • Most strains also secrete a large pore-forming protein called vacA causes large vacuoles to form in cells in vitro.
H pylori: Pathophysio • Host factors: • Genetic polymorphisms; for example, greater levels of expression of the proinflammatory cytokine interleukin-1β (IL-1β) are associated with greater risk of gastric atrophy & subsequent carcinoma &polymorphisms in other genes involved in the host inflammatory response to infection (e.g. IL-10 / TNF-α) may also be important.
H pylori: Pathophysio • In most people H. pylori causes antral gastritis associated with depletion of somatostatin (from D cells)& gastrin release from G cells unchecked by somatostatin. • The subsequent hypergastrinaemia stimulates acid production by parietal cells, but in the majority of cases this has no clinical consequences. • In a minority of patients (perhaps smokers) this effect is exaggerated, leading to duodenal ulceration • The role of H. pylori in the pathogenesis of gastric ulcer is less clear but probably acts by reducing gastric mucosal resistance to attack from acid/pepsin. • In 1% of infected people, H. pylori causes a pangastritis leading to gastric atrophy/ hypochlorhydria,allows bacteria to proliferate within the stomach; these may produce mutagenic nitrites from dietary nitrates, predisposing to the development of gastric cancer
HP Diagnosis: • Urea Breath tests are best because of their accuracy, simplicity & non-invasiveness.
Smoking: • Smoking confers an increased risk of gastric ulcer & to a lesser extent, duodenal ulcer. • Once the ulcer has formed, it is more likely to cause complications& less likely to heal if the patient continues to smoke. • NSAIDs
Acid-pepsin vs mucosal resistance: • Ulcer forms when there is imbalance between aggressive factors, i.e. acid /pepsin & defensive factors, i.e. gastric /duodenal mucosa, bicarbonte, mucosal blood flow* PGs. • Ulcers occur only in the presence of acid /pepsin; never found in achlorhydric as pernicious anaemia& severe intractable PU nearly always occurs in ZES, characterised by very high acid secretion. • Most DU have markedly exaggerated acid secretion in response to stimulation by gastrin& H. pylori leads to hypergastrinaemia. • In GU the effects of H. pylori are more complex&impaired mucosal defence resulting from a combination of HP, NSAIDs&smoking have a more important role.
Gastroduodenal mucosal protection; PG stimulate HCO3 /mucus secretion& increase mucosal blood flow.
Clinical features: • Chronic with spontaneous relapse /remission lasting for decades, if not for life. • DU/GU share common symptoms. • Recurrent abd pain with 3 notable characteristics: epigastric , episodic & relationship to food . • Occasional vomiting occurs in 40%; persistent daily vomiting suggests GOO. • In 1/3 history is less characteristic, esp in elderly on NSAIDs, pain may be absent or slight epigastric unease. • Occasionally, only anorexia / nausea, or a sense of undue repletion after meals. • In some completely 'silent', presenting for the first time with anaemia, abrupt haematemesis or as acute perforation; recurrent acute bleeding. • The diagnostic value of individual symptoms is poor.
Diagnosis: • Endoscopy is the preferred investigation. • Gastric ulcers may occasionally be malignant& therefore must always be biopsied & followed up to ensure healing
Management: • Aims: relieve symptoms, induce healing ,prevent recurrence. • H. pylori eradication is the cornerstone of therapy, as this will successfully prevent relapse& eliminate the need for long-term therapy in the majority. • H. pylori eradication All patients with proven acute or chronic DU &GU who are H. pylori-positive should be offered eradication as primary therapy. • Treatment is PPI simultaneously with two antibiotics (from amoxicillin, clarithromycin , metronidazole) for 7 days. • Success is > 90%, although compliance, side-effects& metronidazole resistance influence the success of therapy. • Second-line therapy should be offered to those patients who remain infected after initial therapy,choice lies between a third attempt with quadruple therapy (bismuth, PPI+ 2 antibiotics) or long-term maintenance therapy with PPI.
Management: • H. pylori / NSAIDs are independent risk factors for ulcer • High risk patients requiring long-term NSAIDs should first undergo eradication therapy to reduce ulcer risk. • This may not be necessary in young, fit patients with no history of ulcer disease or dyspepsia but a 'test & treat' strategy for older patients with major comorbidity or a previous ulcer history is recommended. • Subsequent co-prescription of PPI+ NSAID is advised but is not always necessary for patients being given low-dose aspirin in whom the risk of ulcer complications is lower
COMMON SIDE-EFFECTS OF HP ERADICATION: • Diarrhoea • 30-50%; usually mild but Clostridium difficile-associated colitis can occur. • Flushing & vomiting when taken with alcohol (metronizadole) • Nausea, vomiting • Abdominal cramp • Headache • Rash
Other indications OF HP ERADICATION: • Definite • Peptic ulcer • MALToma • H. pylori-positive dyspepsia • Not indicated • Asymptomatic • Gastro-oesophageal reflux disease • Uncertain • Family history of gastric cancer • Non-ulcer dyspepsia • Low risk Long-term NSAID users
General measures: • Cigarette smoking, aspirin/ NSAIDs should be avoided. • Alcohol in moderation is not harmful. • No special dietary advice is required. • Short-term management: many different drugs are available for of acid peptic symptoms. • Maintenance treatment: Continuous maintenance treatment should not be necessary after successful H. pylori eradication. • For the minority who do require it, the lowest effective dose should be used.
Misoprostol Ranitidine + _ _ _ _ _ + + + + + + + Omeprazole Antacid PGE2 Gastrin Histamine Proglumide ACh H2 M3 Adenyl cyclase Gastrin receptor PGE receptor Ca++ ATP cAMP Ca++ Protein Kinase (Activated) K+ H+ K Parietal cell Proton pump Lumen of stomach Gastric acid
Surgery: • The cure of most peptic ulcers by H. pylori eradication & availability of safe, potent acid-suppressing drugs have made elective surgery for PUD a rare event
Complications: • Perforation • Ggastric outlet obstruction • Bleeding
PEPTIC ULCER DISEASE IN OLD AGE: • Gastroduodenal ulcers: have a greater incidence, admission rate & mortality. • Causes: high prevalence of H. pylori & NSAID use& impaired defence mechanisms. • Atypical presentations: pain &dyspepsia are frequently absent or atypical so older people develop complications such as bleeding or perforation more frequently. • Bleeding: older patients require more intensive management (including central venous pressure measurement) than younger patients because they tolerate hypovolaemic shock poorly.