Download
1 / 123
1.68k likes | 2.96k Views
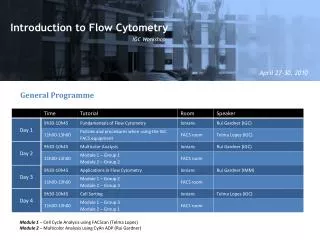
Flow Cytometry in Haematology. APPLICATIONS. Diagnosis, subtyping of lymphoproliferative disorders & leukaemias Detection of residual disease in above CD34 assays Lymphocyte subsets PNH studies Foeto-maternal hemorrhage DNA Ploidy, Apoptosis Platelet aggregation. PNH.

E N D
APPLICATIONS • Diagnosis, subtyping of lymphoproliferative disorders & leukaemias • Detection of residual disease in above • CD34 assays • Lymphocyte subsets • PNH studies • Foeto-maternal hemorrhage • DNA Ploidy, Apoptosis • Platelet aggregation
PNH • Although Ham’s test and Sucrose lysis tests are sensitive & specific, their accuracy is strongly operator dependent and are cumbersome (HT). • Principle of FCM: Absent or markedly diminished expression of glycosyl phosphatidylinositol-anchored protein (GPI-AP) on red cells and/or white cells in the appropriate clinical setting. • GPI-AP - CD59 (MIRL) & CD55 (DAF) • Use two GPI-AP for confirmation
PNH • Can detect small clones in multiple lineages but red cells usually adequate; granulocyte analysis ? technically more challenging & need to be tested immediately. • Quantify clone size (down to 0.1%) • Granulocytes not influenced by haemolysis or transfusion but the red cell testing is reliable even with significant transfusion. • Obviously the % of abnormal red cells would be affected by both above factors
PNH • A more sensitive assay (0.004%) using a bacterial toxin-aerolysin which spares PNH cells • Red cells show clearest delineation between phenotypes • Assay both erythrocytes and granulocytes • Small proportion (esp PNH/AA) may only be detected on granulocyte clones
PNH • Summary: Analysis of GPI-AP – highly specific test for PNH. • No other disease in which the erythrocytes are a mosaic of both GPI-AP+ & GPI-AP- cells • Patients with isolated deficiency of either CD59 or CD55 are extremely rare & in those cases 100% of cells are abnormal & expression of only one GPI-AP is deficient
CD34 assays • CD34 – surrogate marker of hemopoietic progenitor cells • 0.1% of PB mononuclear cells & 1-3% of human bone marrow cells • Various antibodies available • Prefer PE conjugated ab because of the rarity of these cells
CD34 assay • Method (ISHAGE- ISCT) - Sequential gating to define CD45+cells (low to intermediate), CD34+ & with side scatter similar to blast cells • + viability using 7 AAD • RMH - ISHAGE CD34 Coulter Stem Kit Enumeration Method • 3 RCPA- QAP surveys each year
CD34 assay • CD34 cell count in an autograft correlates well with the rate of hemopoietic recovery. • Values of 2-5x106 cells/kg predicting rapid & durable engraftment following PBSCT. • It has been demonstrated in one study that a PB CD34+ cell count of > 5.0x106/lpredicts a satisfactory harvest. • Before apheresis WBC > 5x109/l and blood CD34 conc. > 1x 104/ml
ANZSBT Guidelines for Laboratory Assessment of Fetomaternal Haemorrhage1st edition - 2002 • Summary & Recommendation • Page 6 Section 3. • “Flow cytometry is accepted as the most accurate quantitative test for FMH…The Scientific Sub-Committee believes this is the method of choice for quantitation if readily available”
Example of calculation of FMH volume using flow method • Foetal cells assumed to be 22% larger than maternal cells • Assumed average maternal red cell volume of 1800 ml • E.g. for flow result of 0.5% foetal red cells • Uncorrected foetal RBC vol: 1800 x 5/1000 = 9 • Corrected for foetal RBC vol: 9 + (9 x 22/100) = 10.98 ml
Revised Guidelines on Immunophenotyping in Acute Leukaemias and Chronic Lymphoproliferative Disorders. BSH: Clinical & Laboratory Haematology 2002;24:1-13.
Background • Major technical advances • Improved instrumentation • New monoclonal antibodies • Up to 6 colour staining • Permeabilizing agents • CD45 gating strategies
Pre-analytical factors • Blood and bone marrow samples • Anticoagulant (EDTA or Heparin) • Specimen to be analysed within 24 hours • Storage at 2-200C • No need to isolate mononuclear cells • Care with lysing procedure
General Recommendations • Immunophenotyping should be assessed in conjunction with clinical features and cell morphology. • Need for Quality System Essentials to be adhered to.
Selection of FluorochromesRuiz-Arguelles et al Clinical Cytometry, 70B, 39-44, 2005 • Abs whose normal expression is rather dim (eg CD7, CD10, CD11b, CD13, CD2, CD34, CD64, CD117 or TdT) should be labelled with the most bright fluorochromes: phycoerythrin and, if instrumentation allows, allophycocyanin.
LEUKEMIA IMMUNOPHENOTYPING STRATEGY • Identify blasts/abnormal cells • Determine lineage (B, T-lymphoid or myeloid) • Determine immunological subtype (EGIL) • Search for leukemia aberrant phenotypes • Customise follow up panel for MRD
Reporting FCM results • Should include: • Light scatter properties • Presence or absence of each of tested ags • Intensity, modality or coexpression of ags • Description of the normal cell population • For MRD, the estimated number of malignant cells
The value of autoflourescence as a diagnostic feature of APML • Hayden et al, Dublin, Haematologica 2006;91:417-418
New disease identification/classification • T-CD4+ (CD56+, CD57+, TCRab+) : a new clonal T-LPD (San Miguel 2004) • 2% of LPD • no cytopenias • no AID • frequently associated with neoplasia • CD4+ CD56+ lin- pDC leukemia • a new entity, 1st reported by GEIL in 2002 • Elderly, Cutaneous lesions, CNS disease common • Initial CR common but then aggressive relapse • Only 25% 2 year survival
Monoclonal B lymphocytes with the characteristic of “indolent” CLL are present in 3.5% of adults with normal blood counts • Rawstron A et al. Leeds, UK • Blood 15 July 2002
The Natural History of “Early CLL”Rawstron et alBlood ASH 2003 #656 • Progression to clinically relevant disease with ~ 1% annum requiring treatment • Identifying an absolute cut-off for diagnosis is less clinically relevant than identifying the specific cell phenotype & genotype
Monoclonal CD5+ and CD5- B-lymphocyte expansions are frequent in the peripheral blood of the elderly • Paolo Ghia et al Multicentre, Italy • Blood March 15, 2004
The question we are facing is whether the presence of monoclonalB cells in the PB of otherwise healthy subjects may have a clinicalbearing and if so, to what extent. The results of the presentstudy call for increased caution in interpreting FCMresults in a clinical setting. The widespread use of the evaluationof the / ratio, during common diagnostic procedures, suggeststhat clinically silent circulating B-cell clones may be rathereasily reported during routine controls, bringing along thedifficulty of the interpretation in terms of clinical prognosis.Prospective studies are definitely needed in order to definethe features, if any, that can discriminate between "benignB-cell clones" and "progressive B-cell clones" as well as toidentify those individuals who would benefit from clinical followup. The experience with MGUS suggests that this may be a clinicalresult quite difficult to reach.
Immunophenotyping of Leukaemias Using a Cluster of Differentiation Ab Microarray:Belov et al Cancer Research June 2001 • Suspension of cells is applied to an array of >50 abs on a glass slide • Enables concurrent determination of > 50 antigens
Exp 4/2005 Diagnostic kit Software Embedded algorithm compares captured image with proprietary database of consensus binding patterns Nanoarray plus other consumables Medsaic Immunomicroarray Nanoarray Scanner Proprietary slide reader capture image and transfers this file to attached PC Glass slide with immobilised capture molecules specific for each discriminatory marker • Full proteomic analysis • Detailed diagnostic report
Immunomicroarray (contd) • Advantages: • Test for many more antigens. • Simple technique • No flow cytometer required • Disadvantages: • Multiparameter studies not possible • Various cell populations can’t be separated • Antigen co-expression
B lymphoid development CD34 CD22
T lymphocyte development CD34 CD3