Download
1 / 34
370 likes | 468 Views
Explore the anatomy of spinal nerve roots, their relation to vertebral structures, regions of innervations, and common clinical disorders. Learn about spinal cord endings, vertebral structures, disc herniations, dermatomes, myotomes, and radiculopathy symptoms.

E N D
Chapter 8Spinal Nerve Roots Abdullah Al-Salti R2 24 February 2010
Outline: • The anatomy of the spinal nerve roots . • Their relation to the vertebral structures. • Regions of innervations . • Common clinical disorders.
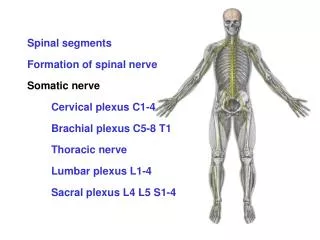
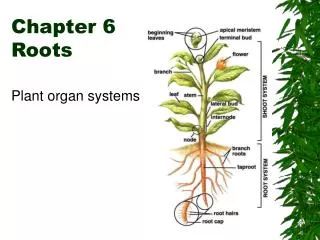
Anatomy Of The Spinal Nerve Roots • 31 pairs spinal nerves: There are 8 cervical (C1-C8),12 thoracic (T1-T12),5 lumber (L1-L5),5sacral(S1-S5)and 1coccygeal(Co1)spinal segments. • Formation: each spinal nerve is formed by union of anterior and posterior roots at intervertebral foramen • The anterior root-contains motor fibers for skeletal muscles. Those from T1 to L2 contain sympathetic fibers; S2 to S4 also contain parasympathetic fibers. • The posterior root-contains sensory fibers whose cell bodies are in the spinal ganglion.
General Description • In adults , the spinal cord normally ends with the conus medullaris at the level of the L1 or L2 vertebral bones. • The roots of the cauda equina are organized such that the most centrally located roots are from the most caudal segments of the spinal cord. • Sensory and motor nerve roots arise from each segment of the spinal cord except for the C1 and Co1 segments,which have no sensory roots. • The cervical enlargements (C5-T1)gives rise to the nerve roots for the arms ,and the lumbosacral enlargments (L1-S3)gives rise to the nerves roots for the legs.
Vertebral Structures. • Each vertebral bone has a sturdy cylindrical vertebral body located anteriorly. • Posteriorly,the neural elements are surrounded by an arch of bone formed by the (pedicles,transverse processes,laminae,and spinous processes). • The superior and inferior articular processes or facet joints form additional points of mechanical contact between adjacent vertebrae. • Intervertebral disc (nucleus pulposus surrounded by annulus fibrosis).
General Description • The spinal cord runs through the spinal canal (vertebral foramen) and is surrounded by pia,arachnoid ,dura mater . • Unlike in the cranium , there is a layer of epidural fat between the dura and the periosteum in the spinal canal,which is a useful landmark on MRI scans. • There is a valveless meshwork of epidural veins called Batsons plexus that is thought to play a role in the spread of metastatic cancers and infections in the epidural space. • Ligamentum flavum is particularly prominent in cervical and lumber regions and can sometimes become hypertrophied and contribute to spinal cord or nerve root compression. • The nerve roots exit the spinal canal via the neural (intervertebral) foramina.
General Description • Disc herniation are most common at the cervical and lumbosacral levels. • For both cervical and lumbosacral disc herniations, the nerve root involved usually corresponds to the lower of the adjacent two vertebrae. Example C5-C6 and L5-S1. • Cervical discs are usually constrained by the posterior longitudinal ligament to herniate laterally toward the nerve root, rather than centrally toward the spinal cord.
General Description • Thoracic ,lumber and sacral nerve roots exit below the correspondingly numbered vertebral bone.Cervical nerve roots,on the other hand, exit above the correspondingly numbered vertebral bone, except for C8 exit between C7 and T1. • The lumosacral nerve roots exit some distance above the intervertebral discs.As they are about to exit, the nerve roots move into the lateral recess of the spinal canal and at this point that they are closest to the disc.
General Description • Posterolateral disc herniations in the lumbosacral spine ,usually impinge on nerve roots on the lower vertebral bone. • Far lateral disc herniation result in impingement of the next higher nerve root. • Central disc herniation ,at the level of cauda equina can impinge on nerve roots lower than the level of herniation.
Dermatomes and myotomes. Dermatomes: • The sensory region of the skin innervated by a nerve root. • Most of the head is supplied by C2 , via the greater and lesser occipital nerves. • Common land marks ,T4, T10 ,T12. • There is a skip between C4 and T2, with C5 through T1 represented on the upper extremities. • There is considerable overlap between adjacent dermatomes. Myotome: The muscles innervated by a single nerve root.
Radiculopathy • Pain and paresthesias (burning, tingling pain that radiates or shoots down the nerve root ),radiating in the distribution of a nerve root, often associated with sensory loss and paraspinal muscle spasm • Sensory loss (often vague or ill defined) • Weakness (often subjective, not present, or mild) • Reflex loss (may be present or absent) • Chronic radiculopathy can result in atrophy and fasciculations. • T1 ---- Horner's syndrome . • Herniated disk is by far the most common cause. • Inflammation is important as a pain mechanism: • Phospholipase A and E, NO, TNF, other pro-inflammatory mediators are released by a herniated disk • The dura surrounding the ventral and dorsal nerve root is bathed in this exudate • Inflammation or prior injury to nerve root is necessary to cause compression to generate continued pain
Diagnostic Test • Valsalva • Cough, laughter, voluntary contraction of abdominal wall muscles, when straining, make radicular pain worse • Stretching the involved nerve root —L5S1—sitting worsens, C5C6—abduct arm over head relieves. • Straight leg raising test.—L5S1 worsens.(10-60). • Crossed straight-leg raising test. specificity over 90% for lumbosacral nerve root compression. • Percussion of the spine. May indicate metastatic disease ,epidural abscess,osteomyelitis,or other disorders of the vertebral bones, although this sign is often absent in these conditions.
Imaging: Modalities X-rays: most useful in trauma to exclude fracture, not sensitive for nerve root or spinal cord pathology. CT: most useful study for bony anatomy. MRI: most useful study for imaging disk, nerve root and spinal cord pathology. Contrast is used if patient has had prior spine surgery in the affected area b/c can light up scar tissue, or if tumor, infection, or other inflammatory etiology is suspected. CT myelogram, CT/w dye injected into spine: in patients who cannot obtain MRI, often the best study for imaging the nerve roots of a selected area. Other diagnostic modalites: EMG and NCS In patients with acute radiculopathy, EMG studies will not be of value until at least 3 weeks . EMG studies can help the decision making process by identifying the distribution and extent of spinal nerve root damage, the degree of acute axon loss, and the likelihood of conduction block.
Treatment of Radiculopathy: Natural history of lumbosacral and cervical radiculopathy: Up to 75% spontaneously improve Length of time required for improvement may be several weeks or up to years! If there is a progressive neurologic deficit or intractable pain, surgical referral is appropriate ,otherwise, most patients can avoid surgery
Empiric Treatment of Radiculopathy: Medications: Pain control with NSAIDS and narcotic medications as necessary Short course of corticosteroids in selected patients; justification is to decrease inflammation around the nerve root. Gentle physical therapy (mobilization and stretching) Bed rest heating pads, ultrasound, gentle massage Traction for the cervical spine Epidural steroid injections for the LS spine Risks are higher in cervical spine Transforaminal steroid injections for the LS spine
Cauda equina and conus medullaris Syndromes: Large midline disk herniation can cause symptoms in both legs in the distribution of multiple nerve roots, bilateral symptoms with large full bladder Cauda equina syndrome: multiple nerve roots bilaterally are affected below the end of the spinal cord at L1-2 Conus medullaris syndrome: the end of the spinal cord from about T11-L1
Cauda equina and conus medullaris Syndromes: Both are potentially surgical emergencies depending on the cause Warning signs that one of these may be present are: Rapidly progressive bilateral lower extremity weakness Saddle anesthesia Loss of ability to urinate voluntarily with a large bladder and overflow incontinence Loss of rectal tone
Cauda Equina and conus medullaris Differentiating the two is difficult, and they may coexist: Cauda equina: More pain, asymmetric at onset, bladder dysfunction not initially as severe. more of lower motor neuron signs Conus medullaris: Often little pain, symmetric at onset, severe bladder dysfunction. more of upper motor neuron signs Key points: Emergent imaging with MRI is essential Make sure to image high enough to see the full conus! To at least T10
References : • Main reference : Neuroanatomy through clinical cases. HAL BLUMENFELD, M.D., PhD. • Other references: Cervical and low back pain and radiculopathy. Jenice Robinson, MD Assistant Professor of Neurology Penn State College of Medicine NBS725 January 12, 2009. DISEASES OF THE NERVE ROOTS Kerry Levin 2008, American Academy of Neurology SPINAL CORD ANATOMY, LOCALIZATION, AND OVERVIEW OF SPINAL CORD SYNDROMES Gregory Gruener, Jose´ Biller 2008, American Academy of Neurology Human Anatomy, First Edition McKinley & O'Loughlin Lumbar Disc Herniation and Radiculopathy KS Hospital Spine Center
END Spinal Nerve Roots Abdullah Al-Salti R2 24 February 2010