Download
1 / 1
10 likes | 157 Views
Pre-procedural INR: Does It Matter?. Heather Figurelli, DO; Naser Khan, MD; Baseer Qazi, MD; Dean Silas, MD Department of Medicine, Division of Gastroenterology Advocate Lutheran General Hospital. Discussion:

E N D
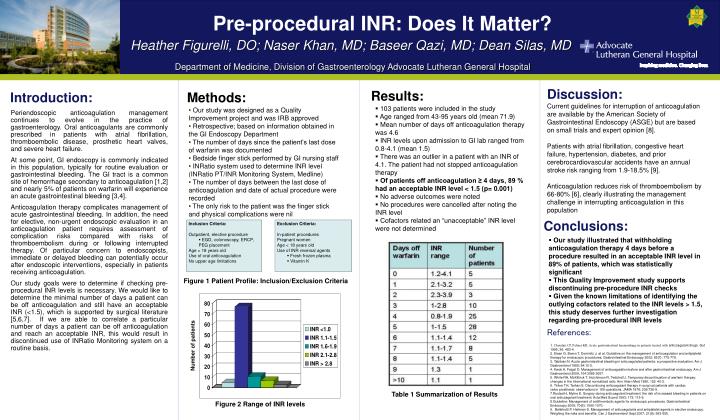
Pre-procedural INR: Does It Matter? Heather Figurelli, DO; Naser Khan, MD; Baseer Qazi, MD; Dean Silas, MD Department of Medicine, Division of Gastroenterology Advocate Lutheran General Hospital Discussion: Current guidelines for interruption of anticoagulation are available by the American Society of Gastrointestinal Endoscopy (ASGE) but are based on small trials and expert opinion [8]. Patients with atrial fibrillation, congestive heart failure, hypertension, diabetes, and prior cerebrocardiovascular accidents have an annual stroke risk ranging from 1.9-18.5% [9]. Anticoagulation reduces risk of thromboembolism by 66-80% [6], clearly illustrating the management challenge in interrupting anticoagulation in this population Results: Introduction: Methods: • 103 patients were included in the study • Age ranged from 43-95 years old (mean 71.9) • Mean number of days off anticoagulation therapy was 4.6 • INR levels upon admission to GI lab ranged from 0.8-4.1 (mean 1.5) • There was an outlier in a patient with an INR of 4.1. The patient had not stopped anticoagulation therapy • Of patients off anticoagulation ≥ 4 days, 89 % had an acceptable INR level < 1.5 (p= 0.001) • No adverse outcomes were noted • No procedures were cancelled after noting the INR level • Cofactors related an “unacceptable” INR level were not determined • Our study was designed as a Quality Improvement project and was IRB approved • Retrospective; based on information obtained in the GI Endoscopy Department • The number of days since the patient’s last dose of warfarin was documented • Bedside finger stick performed by GI nursing staff • INRatio system used to determine INR level (INRatio PT/INR Monitoring System, Medline) • The number of days between the last dose of anticoagulation and date of actual procedure were recorded • The only risk to the patient was the finger stick and physical complications were nil Periendoscopic anticoagulation management continues to evolve in the practice of gastroenterology. Oral anticoagulants are commonly prescribed in patients with atrial fibrillation, thromboembolic disease, prosthetic heart valves, and severe heart failure. At some point, GI endoscopy is commonly indicated in this population, typically for routine evaluation or gastrointestinal bleeding. The GI tract is a common site of hemorrhage secondary to anticoagulation [1,2] and nearly 5% of patients on warfarin will experience an acute gastrointestinal bleeding [3,4]. Anticoagulation therapy complicates management of acute gastrointestinal bleeding. In addition, the need for elective, non-urgent endoscopic evaluation in an anticoagulation patient requires assessment of complication risks compared with risks of thromboembolism during or following interrupted therapy. Of particular concern to endoscopists, immediate or delayed bleeding can potentially occur after endoscopic interventions, especially in patients receiving anticoagulation. Our study goals were to determine if checking pre-procedural INR levels is necessary. We would like to determine the minimal number of days a patient can be off anticoagulation and still have an acceptable INR (<1.5), which is supported by surgical literature [5,6,7]. If we are able to correlate a particular number of days a patient can be off anticoagulation and reach an acceptable INR, this would result in discontinued use of INRatio Monitoring system on a routine basis. Conclusions: • Inclusion Criteria: • Outpatient, elective procedure • EGD, colonoscopy, ERCP, PEG placement • Age > 18 years old • Use of oral anticoagulation • No upper age limitations • Exclusion Criteria: • In-patient procedures • Pregnant women • Age < 18 years old • Use of INR reversal agents • Fresh frozen plasma • Vitamin K • Our study illustrated that withholding anticoagulation therapy 4 days before a procedure resulted in an acceptable INR level in 89% of patients, which was statistically significant • This Quality Improvement study supports discontinuing pre-procedure INR checks • Given the known limitations of identifying the outlying cofactors related to the INR levels > 1.5, this study deserves further investigation regarding pre-procedural INR levels Figure 1 Patient Profile: Inclusion/Exclusion Criteria References: Number of patients • 1. Choudari CP, Palmer KR. Acute gastrointestinal haemorrhage in patients treated with anticoagulant drugs. Gut 1995; 36: 483-4. • 2. Eisen G, Baron T, Dominitz J, et al. Guideline on the management of anticoagulation and antiplatelet therapy for endoscopic procedures. Gastrointestinal Endoscopy 2002; 55(7): 775-779. • 3. Tabibian N. Acute gastrointestinal bleeding in anticoagulated patients: a prospective evaluation. Am J Gastroenterol 1989; 84:10-2. • 4. Kwok A, Faigel D. Management of anticoagulation before and after gastrointestinal endoscopy. Am J Gastroenterol 2009; 104:3085-3097. • 5. White RH, McKittrick T, Hutchinson R, Twitchell J. Temporary discontinuation of warfarin therpay: changes in the international normalized ratio. Ann Intern Med 1995; 122: 40-2. • 6. Tinker TH, Tarhan S. Discontinuing anticoagulant therapy in surgi cal patients with cardiac • valve prosthesis: observations in 180 operations. JAMA 1978; 239:738-9. • Rustad H, Myhre E. Surgery during anticoagulant treatment: the risk of increased bleeding in patients on oral anticoagulant treatment. Acta Med Scand 1963; 173: 115-9. • Guideline: Management of antithrombotic agents for endoscopic procedures. Gastrointestinal Endoscopy 2009; 70(6): 1060-1070. • 9. Belletrutti P, Heitman S. Management of anticoagulants and antiplatelet agents in elective endoscopy. Weighing the risks and benefits. Can J Gastroenterol Sept 2007; 21(9): 553-555. Table 1 Summarization of Results Figure 2 Range of INR levels