Download
1 / 15
150 likes | 290 Views
Overview of the Medicare Drug Benefit. Presented by Tricia Neuman, Sc.D. Vice President and Director, Medicare Policy Project The Henry J. Kaiser Family Foundation for Pfizer Pro Bono Access to Healthcare Conference August 11, 2005. Exhibit 1. Medicare Rx Benefit.

E N D
Overview of the Medicare Drug Benefit Presented byTricia Neuman, Sc.D. Vice President and Director, Medicare Policy ProjectThe Henry J. Kaiser Family FoundationforPfizer Pro Bono Access to Healthcare Conference August 11, 2005
Exhibit 1 Medicare Rx Benefit Phase 1: Transitional Discount Drug Card Program • Medicare-approved discount drug cards available June 2004 • 6.3 million beneficiaries enrolled as of July 2005 • $600 credit in 2004 and 2005 for low-income less than 135% poverty without Medicaid (no asset test) • 1.9 million (of ~7.2 million eligible ) receiving credit • Phases out December 31, 2005 • Can use remaining credit in ‘06 if not in Medicare Rx plan Phase 2: Medicare Prescription Drug Benefit • Begins on January 1, 2006
Exhibit 2 The Basics • Beneficiaries have the choice of: • Traditional, fee-for-service Medicare and receiving drug-only coverage through private prescription drug plans (PDPs) OR • Medicare HMO or PPO for basic benefits and prescription drugs (“Medicare Advantage” drug plans; MA-PDs) OR • Not enrolling in Medicare drug plan • New Medicare drug plans provide “standard” prescription drug benefit or actuarial equivalent • Premium and cost-sharing assistance available for those with incomes below 150% of poverty and modest assets • Medicaid drug coverage terminates December 31, 2005; full-benefit duals transition to Medicare plans by January 1, 2006 • Enrollment period from November 15, 2005 – May 15, 2006 • In the future, Nov. 15- Dec. 31
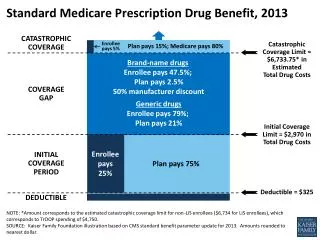
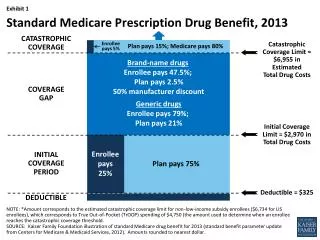
Exhibit 3 Standard Medicare Drug Benefit, 2006 Beneficiary Out-of-PocketSpending 5% Catastrophic Coverage Medicare Pays 95% $5,100 in Total Drug Costs** $2,850 Gap: Beneficiary Pays 100% Gap in Coverage (the “doughnut hole”) $2,250 in Total Drug Costs* Partial Coverage up to Limit Medicare Pays 75% 25% $250 Deductible + ~$450 average annual premium *$2,250 in total spending is equivalent to $750 in out-of-pocket spending. **$5,100 in total spending is equivalent to $3,600 in out-of-pocket spending. SOURCE: Kaiser Family Foundation analysis of Medicare Prescription Drug, Improvement, and Modernization Act of 2003.
Exhibit 4 Overview of Low-Income Part D Drug Benefits, 2006 Note: Cost-sharing subsidies paid by CMS count toward the out-of-pocket threshold. SOURCE: Kaiser Family Foundation summary of Part D low-income subsidies in 2006.
Exhibit 5 Part D and Other MMA Signal More Fundamental Change in Medicare • Big changes expected for Medicare “markets” • Many expect proliferation of new plans: PDPs, MA-PDs (HMOs and PPOs), and private fee-for-service plans • More “players” involved in education/marketing/sales/etc. • Described by some as national test of “consumer-driven” model • Big changes for beneficiaries • Voluntary drug benefit – but with “opt in” rather than “opt out” (unlike Part B) and with penalty for late enrollment • Complex decisions – which may need to be made annually • New annual lock-in • MMA introduces Medicare income/asset tests • Low-income subsidies – administered by Medicaid and SSA (2006) • New income-related Part B premium (2007)
Exhibit 6 The “Right” Choice Will Depend on Many Factors, Including Current Source of Coverage Medigap Medicaid No Drug Coverage Medicare Savings Programs Veterans Employer-Sponsored Coverage State Pharmacy Assistance Program Indian Health Service Medicare- Approved Drug Discount Card Medicare Advantage AIDS Drug Assistance Program TRICARE
Exhibit 7 29 Million Expected to Participate in 2006 Projected Part D Participants: 29.3 million Not Participating in Part D:13.8 million Total = 43.1 Million Medicare Beneficiaries (2006 estimate) Note: *Other non-participants includes federal retirees with drug coverage through FEHBP or TRICARE, and those who lack drug coverage. **Other low-Income includes non dual eligibles with incomes <150% FPL. SOURCE: HHS OACT, MMA Final Rule, January 2005.
Exhibit 8 Projected Reduction in Out-of-Pocket Drug Spending Under the Medicare Drug Benefit, 2006 Medicare Drug Plan Enrollees Who Receive Low-Income Subsidies All Other Medicare Drug Plan Enrollees Average Change:- 37% SOURCE: Actuarial Research Corporation analysis for the Kaiser Family Foundation, November 2004.
Exhibit 9 Issues for Full Benefit Dual Eligibles (6.3 million) Key Provisions • Medicaid stops paying for Rx Dec. 31, 2005 • Auto-enrolled in Medicare Rx plans by HHS - Fall 2005 • In plans at or below average • Medicare Rx coverage begins Jan. 1, 2006 • Can switch plans during year Key Issues • Gaps in coverage • Will drugs be covered • Choice of plans • Will states wrap? SOURCE: MCBS 2002 Access to Care File.
Exhibit 10 Issues for Other Low-Income Beneficiaries (Non-Duals) (8.1 million) Low-income subsidy eligibility and participation: Key Provisions • Apply for subsidy through SSA or Medicaid • Except QMBs, SLMBs, and QI-1s and SSI eligibles - deemed • Reapply at least annually • Must also enroll in Part D plan • Facilitated enrollment for QMBs, SLMBs, QI-1s and SSI, and others determined eligible for low income subsidy – by June 1, 2006 Key Issues • Outreach and enrollment • 2.4 million meet income but not asset test • Choice of plans? Covered drugs? • Different treatment if eligibility determined by Medicaid or SSA 14.4 million Non-Duals expected to qualify based on income and assets 10.9 million <150% FPL; meet asset test <135% FPL; meet asset test Dual Eligibles (auto-enrolled) 6.3 million Dual Eligibles 6.3 million Source: CMS, OACT, MMA Final Rule, January 2005.
Exhibit 11 Participation Rates for Selected Programs Note: Numbers appearing as a range were averaged. Rates for Medicaid and SSI are from 2000 and 2001, respectively. Medicaid take up rates include full benefits and Medicare Savings Programs. SOURCE: Medicaid and SSI rates from GAO, March 2005; QMB and SLMB rates from CBO, July 2004;transitional assistance for the Medicare drug discount card program, HHS 2005.
Exhibit 12 The Clock Is Ticking: Key Dates and Deadlines
Exhibit 13 Two of Three of Seniors Say They Do Not Understand the New Law 68% do not understand the drug law * Don’t know responses not shown. Source: Kaiser Family Foundation Health Poll Report survey (conducted March 31 – April 3, 2005).
Exhibit 14 Minority of Seniors Said They Plan to Enroll in a Medicare Drug Plan in 2006 Yes, will enroll Have not heard enough to decide No, will not enroll Don’t Know/Refused SOURCE: Kaiser Family Foundation Health Poll Report survey (conducted March 31 – April 3, 2005).