Download
1 / 12
120 likes | 269 Views
BioINequivalence: Concept and Definition. Lawrence X. Yu, Ph. D. Director for Science Office of Generic Drugs, OPS, CDER, FDA. ACPS Meeting, October 19-20, 2004. ln Concentration. AUC. Time. Bioavailability: Rate and Extent of Drug Absorption. C max. Concentration.

E N D
BioINequivalence:Concept and Definition Lawrence X. Yu, Ph. D. Director for Science Office of Generic Drugs, OPS, CDER, FDA ACPS Meeting, October 19-20, 2004
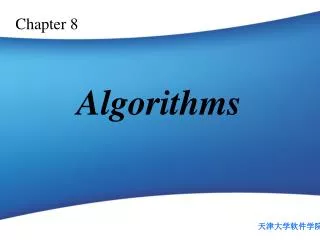
ln Concentration AUC Time Bioavailability: Rate and Extent of Drug Absorption Cmax Concentration Tmax- time of maximum concentration Time
Bioequivalence “the absence of a significant difference in the rate and extent to which the active ingredient or active moiety in pharmaceutical equivalents or pharmaceutical alternatives becomes available at the site of drug action when administrated at the same molar dose under similar conditions in an appropriately designed study…” (21 CFR §320.1)
Bioequivalence • 90% confidence interval for AUC and Cmax between 80-125% • Passing (among others) allows market access • Generic: ANDA approval • Innovator: Demonstrates to be marketed formulation is equivalent to clinical formulation
Why define BioINequivalence? • FDA receives studies that attempt to reverse a previous finding of bioequivalence. • Need standard to evaluate the claim • Published claims of BioINequivalence
What Should Bioinequivalence Mean? • Bioequivalence leads to market access • A study that demonstrates bioequivalence is clear and convincing evidence of equivalence • Bioinequivalence may lead to market exclusion • A study that demonstrates bioinequivalence is clear and convincing evidence of a problem
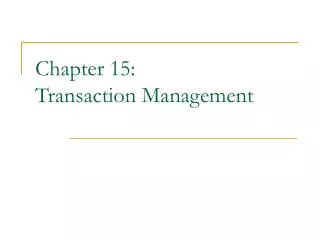
Possible Outcome of BE Studies Demonstrate BE Fail to Demonstrate BIE Fail to Demonstrate BE Demonstrate BIE Demonstrate BIE 80% 125% T/R (%)
Fail to Demonstrate vs. Demonstrate ? Demonstrate BE Demonstrate BIE 80% 125% T/R (%)
Objective • To develop bioinequivalence criteria that are • Scientifically sound • Statistically valid • Fair to all parties • Easy to use
April 14, 2004 ACPS Meeting • Does the ACPS agree with the distinction between demonstrating bioINequivalence and failure to demonstrate bioequivalence? • Committee’s comments: • The Committee felt that there was a need to establish criteria for bioINequivalence evaluation and the criteria should not be just as failure of the bioequivalence test. The members argued it was important to focus on the clinical relevance with the therapeutic index. The Committee discussed both Area under the Curve (AUC) and Cmax as metrics important for bioequivalence and bioINequivalence.
April 14, 2004 ACPS Meeting • Does the ACPS recommend a preferred method for evaluating the three pharmacokinetic endpoints for bioINequivalence? • If bioINequivalence is demonstrated for any one pharmacokinetic endpoint, then bioINequivalence is demonstrated for the products. • BioINequivalence must be demonstrated for all three pharmacokinetic endpoints for bioINequivalence to be demonstrated for the products. • There should be one pre-selected pharmacokinetic endpoint used for bioINequivalence testing. If so, which one? • The three pharmacokinetic endpoints should be evaluated for bioINequivalence with statistical corrections to the level of significance for each endpoint in order to maintain an overall significance level of 0.05.
April 14, 2004 ACPS Meeting • Committee’s comments: • The Committee agreed on a general understanding of bioINequivalence to move forward by recognizing it is not a simple matter. In addition, the members felt this is an important concept, especially how it applies to the entire regulatory scenario. There was no consensus at this point as to a final criteria pertaining to the three pharmacokinetic endpoints.