Download
1 / 15
150 likes | 281 Views
MIMO Clinical Trial. MINIMIZE IMPLANTS, MAXIMIZE OUTCOMES. Patient/Parent/Guardian Education Module. This presentation will describe a research study that you and your family may decide to join.

E N D
MIMO Clinical Trial MINIMIZE IMPLANTS, MAXIMIZE OUTCOMES Patient/Parent/Guardian Education Module
This presentation will describe a research study that you and your family may decide to join. The purpose of this study is to determine how many surgical implants give the best result following scoliosis surgery. MIMO Clinical Trial MINIMIZE IMPLANTS, MAXIMIZE OUTCOMES
Scoliosis Scoliosis is a curvature of the spine. The most common type of scoliosis in children is ‘adolescent idiopathic scoliosis,’ meaning that the causes are uncertain. Scoliosis can become more severe as children and adolescents grow. Even in adulthood, severe scoliosis may continue to worsen by up to one degree per year. This can cause deformity, pain, and in some instances breathing problems.
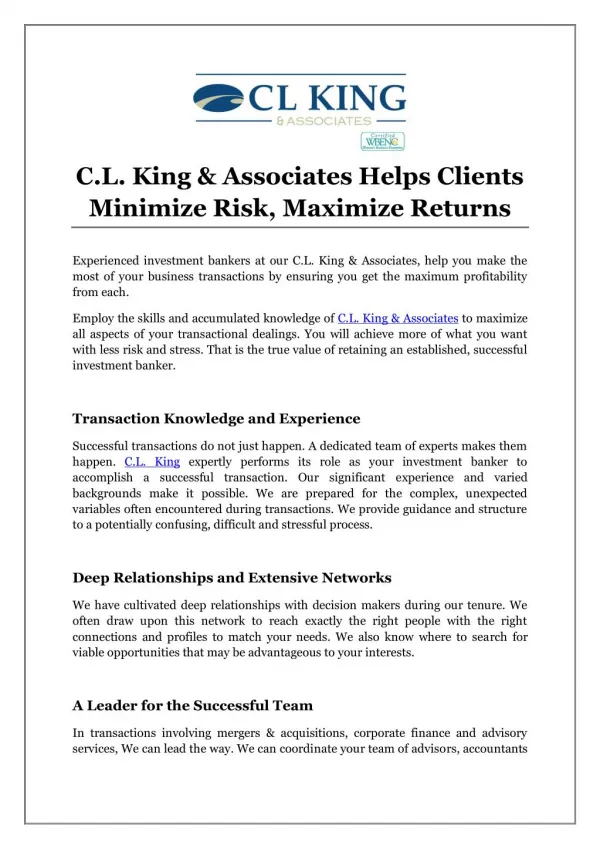
Scoliosis This child has uneven shoulder blades and mild differences in her waist. Mild scoliosis is often only observed. Moderate scoliosis in a growing child can be observed or treated with a brace. For severe scoliosis, doctors often recommend surgery in order to prevent worsening of the curve and to partially straighten the spine.
Surgery for Scoliosis Surgery for scoliosis in adolescence typically involves a fusion, or allowing some of the vertebrae (bones) of the spine to grow together into one solid unit. For fusion to occur, the bones must be held firmly together after surgery. Implants (typically rods, screws and hooks) are used internally to correct the curvature and limit motion of the bones while they heal. These implants are beneath the skin and muscles and typically remain in place permanently.
Surgery for Scoliosis Over the years surgeons have used several types of implants. Today, most scoliosis surgeons attach special screws to the spine to correct the curvature. Many specialists around the country use these implants, called “pedicle screws.” Some surgeons use as many implants as the spine will hold (high density). Other surgeons use implants selectively (low density). It is unknown which approach gives the best result. In fact, there are experienced surgeons using both techniques and achieving very successful surgical results. If you and your family decide to participate in this study, you may help answer this question and improve treatment for children in the future.
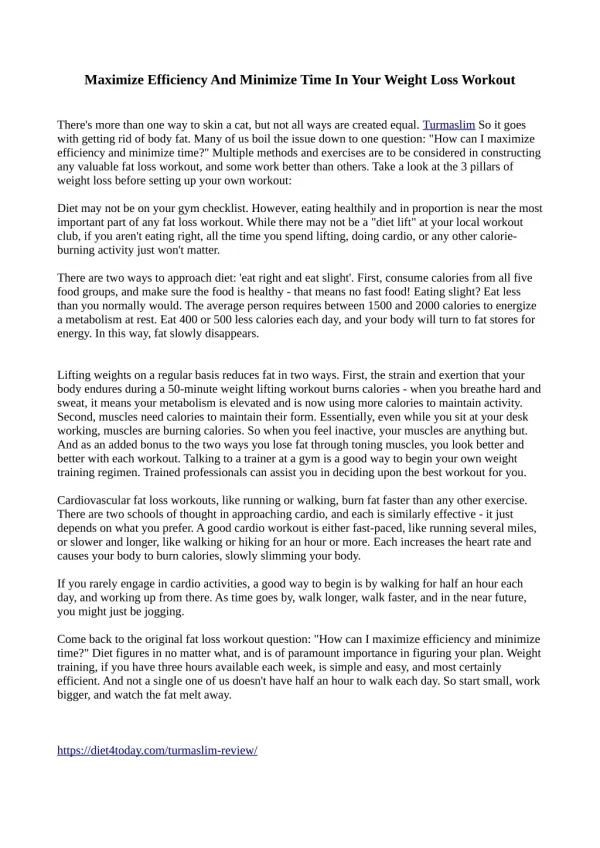
Example of High vs. Low Density Pedicle Screws More Screws Fewer Screws
MIMO Clinical Trial MINIMIZE IMPLANTS, MAXIMIZE OUTCOMES This study has two treatment groups. If you choose to participate, you will be randomly assigned to one of the two groups. Both groups will undergo state-of-the-art care for treatment of scoliosis. One group will have fewer screws used. The other group will have more screws used. There are potential advantages to being in either group. Surgeons across the nation use both approaches. It is uncertain which approach is best.
MIMO Clinical Trial MINIMIZE IMPLANTS, MAXIMIZE OUTCOMES Fewer Screws More Screws
How Many Implants are Needed? The Results of Previous Studies We have studied existing research about whether more screws provide better correction of the spine. Most of the previous studies had few patients. Previous studies suggest that both more screws and fewer screws give good correction and are safe.
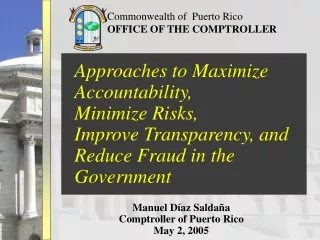
How Many Implants are Needed? The Results of Previous Studies The average curve correction ranged from 64 to 72%. Number of screws spine level fused ranged from 0.8 to 1.81. Study Number % Curve Correction (Red) Number of Screws (Blue)
More About Randomization This study has been designed to randomly assign patients to groups. This is the most powerful way of studying a research question. If the patient or the doctor chooses the treatment, this makes the results of the study less valid and introduces bias into the study. Assigning patients to one of two treatments at random is ethical because both treatments are believed to be equally as effective. Surgeons across the U.S. think that both treatments are safe and equally as good. Further, each hospital has a group of community members and doctors, who have reviewed this study. They also believe that each treatment is safe and equally effective.
More About Randomization Being randomly assigned to the group with more screws or fewer screws used for surgery means that a computer will decide at random which group you will be in. Your surgeons, however, will always have the duty to do what they think will be best for you. At any time, if there is concern that your health will be at risk from the treatment, your surgeons will remove you from the study. At any time, if you or your family decide that you no longer want to be part of the study, you may simply withdraw.
Your Rights as a Patient Please consider your options carefully with your family members. If you do not want to be part of the study, this will not affect the quality of your care. No additional rechecks are necessary as part of this study. You will be asked to complete surveys about how you feel about your treatment at each visit. Your surgeon typically will follow you for many years after surgery. If you do not think you can return in 2 years, then please refrain from joining the study. It is important to have full participation for the 2-year planned rechecks in order to make our study valid. Please ask your care provider or any of these contacts about any additional questions you may have.
Contacts: David Polly, MD pollydw@umn.edu (612) 273-1177 A. Noelle Larson, MD larson.noelle@mayo.edu (507) 284-2995 Charles Ledonio, MD ledon001@umn.edu (612) 273-8035 MIMO Clinical Trial MINIMIZE IMPLANTS, MAXIMIZE OUTCOMES