Download
1 / 1
20 likes | 486 Views
TRIAL OF INSTRUMENTAL VAGINAL DELIVERY IN THEATRE AUDIT Dr Vidya Shirol, Miss Renata Hutt Department of Obstetrics & Gynaecology, Royal Surrey County Hospital NHS Trust , Guildford , UK. INTRODUCTION

E N D
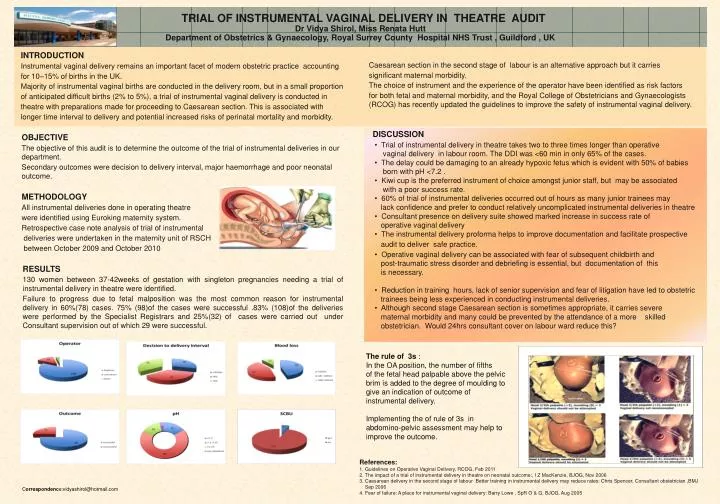
TRIAL OF INSTRUMENTAL VAGINAL DELIVERY IN THEATRE AUDIT Dr Vidya Shirol, Miss Renata Hutt Department of Obstetrics & Gynaecology, Royal Surrey County Hospital NHS Trust , Guildford , UK INTRODUCTION Instrumental vaginal delivery remains an important facet of modern obstetric practice accounting for 10–15% of births in the UK. Majority of instrumental vaginal births are conducted in the delivery room, but in a small proportion of anticipated difficult births (2% to 5%), a trial of instrumental vaginal delivery is conducted in theatre with preparations made for proceeding to Caesarean section. This is associated with longer time interval to delivery and potential increased risks of perinatal mortality and morbidity. Caesarean section in the second stage of labour is an alternative approach but it carries significant maternal morbidity. The choice of instrument and the experience of the operator have been identified as risk factors for both fetal and maternal morbidity, and the Royal College of Obstetricians and Gynaecologists (RCOG) has recently updated the guidelines to improve the safety of instrumental vaginal delivery. OBJECTIVE The objective of this audit is to determine the outcome of the trial of instrumental deliveries in our department. Secondary outcomes were decision to delivery interval, major haemorrhage and poor neonatal outcome. METHODOLOGY All instrumental deliveries done in operating theatre were identified using Euroking maternity system. Retrospective case note analysis of trial of instrumental deliveries were undertaken in the maternity unit of RSCH between October 2009 and October 2010 • DISCUSSION • Trial of instrumental delivery in theatre takes two to three times longer than operative • vaginal delivery in labour room. The DDI was <60 min in only 65% of the cases. • The delay could be damaging to an already hypoxic fetus which is evident with 50% of babies • born with pH <7.2 . • Kiwi cup is the preferred instrument of choice amongst junior staff, but may be associated • with a poor success rate. • 60% of trial of instrumental deliveries occurred out of hours as many junior trainees may • lack confidence and prefer to conduct relatively uncomplicated instrumental deliveries in theatre • Consultant presence on delivery suite showed marked increase in success rate of • operative vaginal delivery • The instrumental delivery proforma helps to improve documentation and facilitate prospective • audit to deliver safe practice. • Operative vaginal delivery can be associated with fear of subsequent childbirth and • post-traumatic stress disorder and debriefing is essential, but documentation of this • is necessary. • Reduction in training hours, lack of senior supervision and fear of litigation have led to obstetric • trainees being less experienced in conducting instrumental deliveries. • Although second stage Caesarean section is sometimes appropriate, it carries severe • maternal morbidity and many could be prevented by the attendance of a more skilled • obstetrician. Would 24hrs consultant cover on labour ward reduce this? RESULTS 130 women between 37-42weeks of gestation with singleton pregnancies needing a trial of instrumental delivery in theatre were identified. Failure to progress due to fetal malposition was the most common reason for instrumental delivery in 60%(78) cases. 75% (98)of the cases were successful .83% (108)of the deliveries were performed by the Specialist Registrars and 25%(32) of cases were carried out under Consultant supervision out of which 29 were successful. The rule of 3s : In the OA position, the number of fifths of the fetal head palpable above the pelvic brim is added to the degree of moulding to give an indication of outcome of instrumental delivery. Implementing the of rule of 3s in abdomino-pelvic assessment may help to improve the outcome. • References: • 1. Guidelines on Operative Vaginal Delivery, RCOG, Feb 2011 • The impact of a trial of instrumental delivery in theatre on neonatal outcome:, I Z MacKenzie, BJOG, Nov 2006 • 3. Caesarean delivery in the second stage of labour Better training in instrumental delivery may reduce rates: Chris Spencer, Consultant obstetrician ,BMJ • Sep 2006 • 4. Fear of failure: A place for instrumental vaginal delivery: Barry Lowe , SpR O & G, BJOG, Aug 2005 Correspondence:vidyashirol@hotmail.com