Download
1 / 29
290 likes | 526 Views
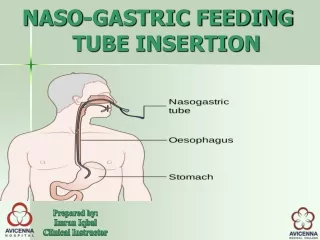
Gastric Tube Placement. Nasogastric. Orogastric. Introduction. What is a gastric tube Anatomy review Indications Contraindications Flight environment Procedure Complications Documentation. Gastric tubes.

E N D
Gastric Tube Placement Nasogastric Orogastric
Introduction What is a gastric tube Anatomy review Indications Contraindications Flight environment Procedure Complications Documentation
Gastric tubes A gastric tube is defined as a tube that is passed into the stomach (Mosby’s:2006) Nasogastric: Insertion via the nose Orogastric: Inserted via the mouth Decompression of the stomach Reduces the risk of aspiration of gastric content Maximises thoracic expansion
Indication: SJA WA Intubated adult patients receiving intermittent positive pressure ventilation in order to facilitate gastric decompression
Indications: General Drug administration Feeding Aspiration of ingested substances Aspiration of gastric content for analysis Upper gastrointestinal bleeding
Contraindications Racoon eyes Nasogastric Radiologically confirmed base of skull fracture (BOS#) Clinical examination indicative of BOS# Bilateral periorbital ecchymosis (racoon eyes) Mastoid ecchymosis (Battles sign) Cerebral spinal fluid leak from nose/ ears Battles sign
Nasal trauma Contraindications Nasogastric Nasal septal deviation or trauma (i.e. middle third facial #) Coagulopathy or systemic anticoagulants Orogastric (combined) Known tracheoesophageal fistula Known oesophageal pathology Caustic or Alkaline ingestion Septal deviation Coagulopathy
Complications: Iatrogenic injury Trauma to nasal, oropharynx and gastrointestinal tract Bleeding (Epistaxis) Perforation of endotracheal tube cuff and loss of IPPV support Bronchial placement leading to atelectasis, pneumonia and lung abscess Bronchial perforation and pleural cavity penetration Pneumothorax Empyema and Sepsis Pulmonary haemorrhage Intracranial penetration
Flight physiology and gastric distention • Gas laws Boyles Law: The volume of a gas is inversely proportional to its pressure when the temperature remains constant P1 X V1 = P2 X V 2 • P1= initial pressure, P2 = final pressure, V1= initial volume and V2= final volume
Practical application (P1) Atmospheric pressure at sea level is 760 mm/hg ( V1) Gastric content is say 100 ml Ascending to 2,438 meters (8000feet) Atmospheric pressure drops to (P2) 565mm/hg To calculate the new volume of gastric content V1 x P1 (760 x 100)= 76000 P2 565 565 New gastric volume 135.5 ml 30% increase Non pressurized aircraft Results: Increased risk of aspiration Splinting of the diaphragm Pain
Equipment Salem Sump nasogastric tube (14-18 French) Tumi 60cc catheter tip syringe Water based lubricant Drainage bag (suction setup if initially on low intermittent suction) Tape PH paper Laryngoscope blade and handle McGills forceps Cophenylcaine spray Optional Tongue depressor Penlight Stethoscope
Features of enteral tubes Regardless of the route of introduction (NGT/OGT) It is recommended that enteral tubes Are radiopaque Have multiple ports (air port) to aid aspiration Have clear centimetre line markers Are made of suitable / choice of materials Have caps attached to close ports when not in use Are available in a number of lengths Are available in a number of sizes
Salem Sump gastric tube: Suction, decompression and irrigation 6-18 French *Can remain in situ 1-3 days Anti Reflux valve: Prevents gastric fluid from exiting the tube via the vent lumen Pressure activated air buffer activates the one way valve when reflux pushes air up the vent lumen Air passes through this one way valve resulting in a “whistle” when placed on suction. Distal end Double lumen PVC tube one for suction the other for sump vent Radio opaque Sump vent equalizes vacuum pressure once gastric content has been emptied. This prevents adhesion to and damage of the gastric mucosa
Procedure: Nasogastric (NGT) BSI and PPE donned Patient meets criteria Consent is obtained Contraindications are excluded Patient is informed of procedure Patient is adequately sedated: analgesia, anxyolitic, paralytics : Nasal cavity is prepared with Cophenylcaine/ lignocaine gel
Procedure: Nasogastric (NGT) Equipment is prepared Gastric tube size is chosen based on patients anatomy (12-16 FR) Tube is measured from the tip of the nose to the tragus of the ear down to the epigastric/ xiphoid region Tube is marked at the proximal end Tube is lubricated with water based lubricant Rt nare is chosen as preferred route of initial entry. Tube is passed into the oesophagus and the stomach via the nasal route. If resistance is met the tube may be rotated clock wise. LT nare is utilized if Access via the RT nare fails
Tragus of the ear Tip of nose Tube is lubricated to facilitate introduction Epigastric/ xiphoid Sizing the nasogastric tube
Procedure: Nasogastric (NGT) Examine the oral cavity during insertion to detect coiling. A tongue depressor and a penlight may help with this procedure *Paralysed and sedated patient will not elicit a gag or cough with inadvertent placement in the lung. For direct esophagoscope the laryngoscope blade is inserted into the oropharynx, the NGT is grasped by the McGills forceps and the tube is guided directly into the oesophagus under direct visualization
Procedure: Orogastric (OGT) • Advantages for orogastric tubes • Excludes risk of epistaxis • Excludes the upper anatomy • Reduction in inadvertent tube collection in the OP • Large opening for introduction of tube Disadvantages More difficult to secure
Procedure: Orogastric (OGT) Initial steps remain the same Tube is measured from the centre of the mouth to the tragus of the ear down to the epigastric / xiphoid process and marked For directesophagoscope the laryngoscope blade is inserted into the oropharynx, the OGT is grasped by the McGills forceps and the tube is guided directly into the oesophagus under direct visualization For indirect insertion • The tongue is held between the thumb and fore finger. The jaw is lifted anterior slightly maintaining spinal alignment • OGT is passed to the back of the OP into the oesophagus and threaded until the pre-marked point is reached
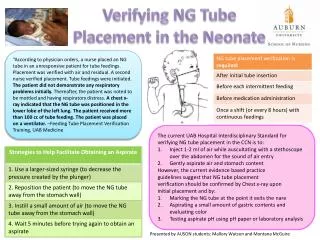
Confirming placement The gold standard is radiological confirmation in the context of secondary retrievals. It is suggested that, where practical, the gastric tube is introduced prior to the CXR that confirms ETT placement. Aspiration of gastric content with subsequent PH test of 5.5 or less. *Gastric PH is influenced by a number of factors including drug administration (PPI,H2 antagonists) When in doubt pull it out ( the tube that is)
Confirming placement Testing methods not to be used: *The ‘Whoosh’ Test:Auscultation of epigastric air entry as air is introduced into the tube via syringe Blue Litmus paper The ‘Bubble’ Test Observing the visual appearance of aspirate February 2005 the NHS National Patient Safety Agency
Radiological confirmation This NGT is in a normal position in the stomach. Erect or supine, AP or PA chest radiography is performed
Radiological confirmation *Basic radiological interpretation of CXR will be covered in another module The NGT is coiled up in the pharynx
Radiological confirmation The tip of the NGT is in the left lower lobe The tip of the NGT is in the right lower lobe
Securing tube Use 2 pieces of hypoallergenic tape approximately 10cm long Tape is split into to pieces from one end to the center Nose is prepared with skin prep or alcohol wipe as needed Tape is applied vertically to the nose. Split ends are crisscrossed around tube Second piece of tape is cut to size and placed horizontally over the first *This procedure will be discussed in the practical skills station Commercial devices may also be used
Post insertion care Once gastric tubes position has been confirmed it is aspirated to remove air and gastric content. The tube is then secured via tape to either the nose or the side of the face The tube is placed into a drainage bag which is secured to the patient (often by safety pins) Visual checks Well secured Signs of migration (curling) External markings Length from nare to tips
Documentation Time and date of procedure Size of tube and route of introduction Method by which tube was confirmed in situ Volume and description of drainage Associated complications as needed