Download
1 / 32
330 likes | 348 Views
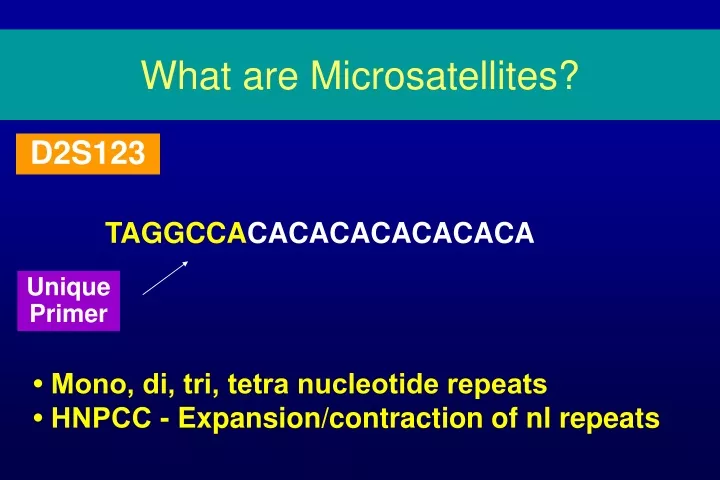
What are Microsatellites?. D2S123. TAGGCCA CACACACACACACA. Unique Primer. • Mono, di, tri, tetra nucleotide repeats • HNPCC - Expansion/contraction of nl repeats. Strand Slippage. D2S123. 14 bp. TAGGCCA CACACACACACACA. 13-15 BP. 4-40 RPTS. Unique Primer. 12 bp.

E N D
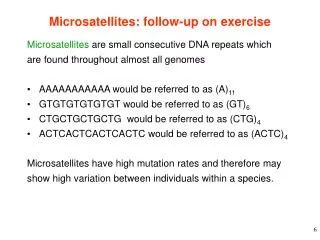
What are Microsatellites? D2S123 TAGGCCACACACACACACACA Unique Primer • Mono, di, tri, tetra nucleotide repeats • HNPCC - Expansion/contraction of nl repeats
Strand Slippage D2S123 14 bp TAGGCCACACACACACACACA 13-15 BP 4-40 RPTS Unique Primer 12 bp TAGGCCACACACACACACACA
Mis-Match Repair Genes • hMSH2 • hMLH1 • PMS1 • PMS2 • hMSH3 • hMSH6
Risk of CRC in ClinicalHNPCC Families: Netherlands Sporadic HNPCC Age 44 69 Location pr: 53% pr: 32% ds: 41% ds: 68% CI35 10% .07% CI50 24% .5% CI75 42% 5.3% Voskuil, Int J CA 1997;72:205
Risk of CRC in MSH2/MLH1HNPCC Families: Netherlands % CRC Lifetime 80 Women 83 Men 92 Endometrial 50 Vasen, Gastro 1996;110:1020
HNPCC • ~ 90% of tumors show MI • Germline defect in MMR genes • 2nd Hit - Somatic Mutation
MSI in Sporadic CRC • 10 - 15% of sporadic CRC • In HNPCC: Germline + somatic = MSI • Sporadic - biallelic somatic mutation via methylation of MLH1 promoter
TC = Transcription Complex Click for larger picture
Gene Testing for hMLH1 or hMSH2 • DGGE • SSCP • IVSP • Direct Sequencing
Gene Testing Cost ($) Sensitivity Sequencing >90% 800 - 3,000 CSGE & Sequencing >90% 1500 Screening (SSCP) 95 - 100% 800 Screening (PTT) 50 - 60% 750 MSI NA 300 Gastro 2001;121:195
Gene Testing for MSH2/MLH1 509 Finnish CRC pts • 5/10 Founder mutation • 7/10 Amsterdam Criteria • All either young, had fam hx, or previous CA 63 MSI 10 (2%) MMR mutations Aaltonen, NEJM 1998;38:1481
Predictive Model for MMR Gene Testing 184 Kindreds: 26% w/ MMR mutations 1) Mean age at diagnosis of affecteds 2) At least 1 member w/ Endometrial CA 3) Amsterdam Criteria Wijnen, NEJM 1998;339:511
Predictive Model for MMR Gene Testing Logistic Model Prob <20% Prob >20% MMR Analysis MSI - + MMR Analysis Nothing Wijnen, NEJM 1998;339:511
Bethesda Criteria and MMR Mutation N=125, “high risk”, Frankfurt, GE Total + BC - BC N 58 (46%) 67 (54%) 125 MSI 17 (29%) 5 (7.5%) 22 (18%) MMR Mutation 11 (65%) 0 (0%) 11 (9%) B1 - B4 46 (79%) Raedle, Ann Int Med 2001;135:566
Bethesda vs. Amsterdam MMR Mutation MSI status Criteria to predict MSI Spec Sens Amsterdam 6/6 27 94 Amsterdam II 8/10 46 90 Bethesda 11/17 77 60 Raedle, Ann Int Med 2001;135:566
Cost Effectiveness of MSI • Decision tree using MSI (Bethesda guidelines) and MMR mutations • 90% CI for cost-effectiveness of screening patients with cancer & relatives: $4,874 - 21,576 / life year gained • Sensitivity analysis - prevalence HNPCC mutation #1 factor Ramsey, Ann Int Med 2001;135:577
Mutations in HNPCC Kindreds • 32 Kindreds (N=38) in Buffalo and Vermont • Amsterdam Criteria 25% Incidence of Mutations MSH2/MLH1: Conclusion: • Molecular basis unknown for many subjects Weber, Cancer Res 1997;57:3798
Effectiveness of Screening in HNPCC • 252 subjects, 22 Families (119 Control, 133 screen) • Colon q3yrs, 1984, 15 yr F/U • Not randomized - declined participation Screen Control OR P CRC 8 (6%) 19 (16%) .4 .01 Mutation + 18% 41% .4 .02 Deaths to CRC 0 8% <.001 Jarvinen, Gastro 2000;118
Colonoscopy in High Risk Individuals 31 HNPCC Families - 232 Individuals 86 (38.6%) underwent colonos-compared to controls Case Control P CA 5 1 Adenomas 29 11 .03 TV/V (#) 11 1 Ad Diam 9.1 5.8 .02 HGD (#) 9 3 Ponz de Leon, CEBP 1998;7:639
Center for Families at Risk for CRC Jan ‘98 - June ‘00 Goal: To develop a registry of high risk families To assemble blood/DNA for research Recruitment: Physician referral, Media, UPCI CA Registry High Risk Definition: Young onset, FDR young onset, Multiple cancers Overall: 83 individuals (76 families)
UPCI Registry 188 Dead Alive 82 106 Agreed 33 26 23 Unavailable Not Interested 11 (5.9%) Young onset cancers - <45, 45-55 Enrolled
High Risk Patients 70 Probands - Complete data, exclude FAP 67.1% High Risk 23 Young Onset (<55) 9 Multiple CA’s 15 Young and Multiple (8 Amsterdam Criteria)
Problems With Center • Lab Support • Integrated Recruitment • Coordinated Approach With Other Cancers
Gene Testing • www.genetests.org • www.nsgc.org