Download
1 / 97
980 likes | 1.45k Views
Empiric Treatment: Pneumonia. Overview of Pneumonia. http://www.virtualrespiratorycentre.com/diseases.asp?did=38. What is pneumonia?.

E N D
Overview of Pneumonia • http://www.virtualrespiratorycentre.com/diseases.asp?did=38
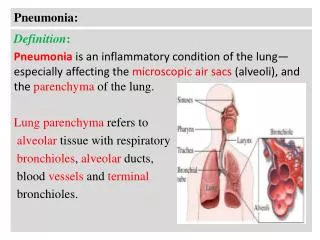
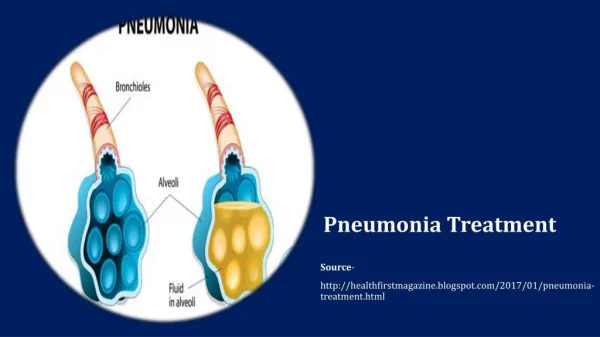
What is pneumonia? • Pneumonia is an inflammatory illness of the lung. Frequently, it is described as lung parenchyma/alveolar (microscopic air-filled sacs of the lung responsible for absorbing oxygen from the atmosphere) inflammation and (abnormal) alveolar filling with fluid.
What Causes Pneumonia? • Pneumonia can result from a variety of causes, including infection with bacteria, viruses, fungi, or parasites, and chemical or physical injury to the lungs.
Pneumonia • The alveoli are tiny air sacs within the lungs where the exchange of oxygen and carbon dioxide takes place.
Bronchiole • Bronchiole: A tiny tube in the air conduit system within the lungs that is a continuation of the bronchi and connects to the alveoli (the air sacs) where oxygen exchange occurs. Bronchiole is the diminutive of bronchus, from the word bronchos by which the Greeks referred to the conduits to the lungs.
Symptoms of Pneumonia • Fever • Chills • Cough • Pleurisy: inflamed membranes around the lungs • Dyspnea: Difficult or labored breathing; shortness of breath
Diagnosis of Pneumonia • Pneumonia usually produces distinctive sounds; these abnormal sounds are caused by narrowing of airways or filling of the normally air-filled parts of the lung with inflammatory cells and fluid, a process called consolidation.
Diagnosis of Pneumonia • In most cases, the diagnosis of pneumonia is confirmed with a chest x-ray. For most bacterial pneumonias, the involved tissue of the lung appears on the x-ray as a dense white patch (because the x-ray beam does not get through), compared with nearby healthy lung tissue that appears black (because the x-rays get through easily, exposing the film). Viral pneumonias typically produce faint, widely scattered white streaks or patches.
Two Types of Pneumonia • Community-Acquired Pneumonia (CAP): individual residing in their homes • Hospital-Acquired Pneumonia (HAP): individuals residing in hospitals
Community-Acquired Pneumonia • Typical: Sudden onset of fever, chills, pleuritic chest pain, productive cough • Streptococcus pneumoniae • Haemophilus influenzae • Atypical: often preceeded by mild respiratory illness • Legionella spp. • Mycoplasma pneumoniae • Chlamydophila pneumoniae
Bacterial Causes of CAP • Streptococcus pneumoniae 16-60% • Haemophilus influenzae 3-38% • Legionella spp 2-30% • Mycoplasma pneumoniae 1-20% • Other aerobic Gram-neg 7-18% • Chlamydophila pneumoniae 6-12% • Staphylococcus aureus 2-5%
Treatment of CAP • Mild • Macrolide (azithromycin, clarithromycin) • Macrolide + -lactam • Doxycycline • Quinolone (moxifloxacin, levofloxacin, gemifloxacin) • Severe • -lactam + macrolide • -lactam + quinolone
Treatment of CAP • Severe • -lactam + macrolide • -lactam + quinolone
HAP is also divided into two classes: • Early onset HAP: occurs within first five days of hospitalization • Late onset HAP: occurs after 5 days of hospitalization
Bacterial Causes ofEarly Onset HAP • Methicillin-sensitive Staphylococcus aureus 29-35% • Haemophilus influenzae 23-33% • Enterobacteriaceae 5-25% • Streptococcus pneumoniae 7-23%
Bacterial Causes of Late Onset HAP • Pseudomonas aeruginosa 39-64% • Acinetobacter spp. 6-26% • Enterobacteriaceae 16-31% • Methicillin-resistant S. aureus 0-2%
Treatment of Early Onset HAP • Ceftriaxone • Quinolone (Levofloxacin, Moxiflocacin, Ciprofloxacin) • Ampicillin/sulbactam • Ertapenem
Treatment of Late Onset HAP Use a combination regimen from the first and second categories below: • Antipseudomonal cephalosporin: ceftazidime, cefepime • Or Carbapenem: Imipenem, Meropenem • Or Extended spectrum penicillin/-lactamase inhibitor: piperacillin/tazobactam ++++ • Quinolone (ciprofloxacin, levofloxacin) • Or Aminoglycoside (gentamicin, tobramycin, amikacin) • If MRSA is suspected, add: Vancomycin or Linezolid
Urinary Tract Infections • http://www.virtualrenalcentre.com/diseases.asp?did=281
Mild and Severe UTI’s • Mild • Involve only the urethra and bladder • Referred to as “acute cystitis” • Symptoms include • dysuria (painful urination) • urinary frequency • hematuria (blood in urine)
Mild and Severe UTI’s • Severe • Infection of the upper urinary tract involves the spread of bacteria to the kidney • Symptoms include fever, chills, nausea, vomiting and flank pain • Called “pyelonephritis”
‘Complicated’ and ‘Uncomplicated’ UTI’s • Uncomplicated: occur in young, healthy, nonpregnant women • Complicated: All other UTI’s
Bacterial Causes of Uncomplicated UTI’s • Escherichia coli 53-79% • Proteus mirabilis 4-5% • Staphylococcus saprophyticus 3% • Klebsiella spp. 2-3% • Other Enterobacteriaceae 3%
Treatment of Uncomplicated Acute Cystitis • Oral trimethoprim-sulfamethoxazole • Oral quinolones (ciprofloxacin, levofloxacin)
Treatment of Uncomplicated Acute Pyelonephritis • Quinolones: Ciprofloxacin, levofloxacin • Third generation cephalosporins: Ceftriaxone, cefotaxime, ceftizoxime • If Gram positive organisms seen in urine: • Aminopenicillin (amoxicillin) • Aminopenicillin + -lactamase inhibitor: (amoxicillin + clavulanate) • Aminopenicillin + aminoglycoside (ampicillin + gentamicin)
Treatment of Complicated Urinary Tract Infections • Fourth generation cephalosporins (cefepime) • Quinolones: Ciprofloxacin, Levofloxacin • If Gram-positive bacteria seen in urine: • Aminopenicillin + aminoglycoside: Ampicillin + gentamicin
Pelvic Inflammatory Disease • http://www.virtualendocrinecentre.com/diseases.asp?did=791
PID is the general term for an infection that has traveled through the vagina, to the uterus, and then to other parts of the pelvis
Symptoms of PID • Abnormal bleeding • Dyspareunia (pain during sexual intercourse) • Vaginal discharge • Lower abdominal pain • Fever • chills
Bacterial Causes of PID • Neisseria gonorrhoeae 27-56% • Chlamydia trachomatis 22-31% • Anaerobic and facultative bacteria (Bacteria that can live under aerobic or anaerobic conditions) 20-78%
Treatment of PID • Mild to Moderate Disease • Oral quinolone: Levofloxacin, ofloxacin + oral metronidazole • Single IM dose of cephalosporin + oral doxycycline + oral metronidazole
Treatment of PID Those that are severely ill should be admitted to the hospital and treated initially with intravenous agents. • Severe Disease (regimen 1) • Cephalosporin with anaerobic activity (cefotetan, cefoxitin) + doxycycline (active against atypical C. trachomatis) • Severe Disease (regimen 2) • Clindamycin (active against C. trachomatis and against many anaerobes) + Gentamicin (effective against Gram-negative N. gonorrhoeae)
Meningitis • http://www.virtualneurocentre.com/diseases.asp?did=162 • http://www.nmaus.org/about_meningitis/index.htm
Meningitis • Meningitis is the inflammation of the protective membranes covering the central nervous system, known collectively as the meninges. Meningitis may develop in response to a number of causes, most prominently bacteria, viruses and other infectious agents, but also physical injury, cancer, or certain drugs.