Download
1 / 11
110 likes | 324 Views
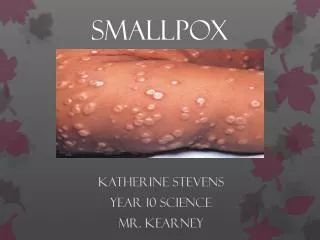
Threat to Fighting Forces. Released as a weapon, smallpox virus would significantly degrade combat mission capability, because almost all troops are susceptible.Outbreak could restrict movement of troops, aircraft, ships. Smallpox would stress medical operations to maximum capacity. . Smallpox.

E N D
1. Smallpox Planning
2. Threat to Fighting Forces Released as a weapon, smallpox virus would significantly degrade combat mission capability, because almost all troops are susceptible.
Outbreak could restrict movement of troops, aircraft, ships.
Smallpox would stress medical operations to maximum capacity.
3. 1776 � American forces too weak from smallpox to capture Quebec:
5,500 smallpox casualties out of 10,000 forces
George Washington ordered variolation of Continental Army against smallpox (archaic procedure, 2% fatal)
1812 � War Department orders Jennerian vaccine substituted for variolation
1919 � Citizens outraged that Woodrow Wilson permits smallpox vaccination of Armed Forces
1980 � WHO declares Earth free of smallpox
1989 � DoD suspends vaccinating U.S. Forces Smallpox Vaccine in History
5. DoD�s special duty to protect: 3.125 M people
Active Duty + Selected Reserve: 2,266,00
Family members + DoD civs overseas: 213,000
Family members residing on base, US: 600,000
625,000 doses of full-strength Dryvax would yield 3.125 M doses, if diluted 1:5
Status of dilution studies
For DoD�s total beneficiary population (including civilian workers) ~ 12 M doses
DoD vaccine requirement: 300K vice 12 M doses
$10 M for phase 1-2 trials, ? lot sizes
6. VIG-IM (IND, �pink�): 4350 vials, ~ 500 treatments @ 1 treatment / 10k vaccinees = 5 M vaccinations
VIG-IV (IND, excess moisture), 350 treatments
$5 M needed to process frozen plasma into ~ 5K units VIG-IV.� DVC subcontract to Massachusetts Biological Laboratories
Restricted to managing vaccine complications, vice prophylaxis of immunodeficient people
DHHS relies on DOD�s VIG for civilian populace, pending CDC RFP for VIG
7. Contingency IND for full-strength Dryvax, in staffing with Joint Staff and Services
IND for VIG, cidofovir in development
Collaboration with CDC (13-15 Mar 02 training)
Brochures, cards, etc: CHPMM, AVIP Agency, __
Electronic signature capture for INDs
www.vaccines.army.mil
www.ind.army.mil
Concept of operations, more specific plans
8. Identify, train teams to respond to outbreak.
JPMPG developing plans
Learn from, leverage, adapt CDC domestic plans to DoD�s global responsibilities.
Request Dryvax from CDC to vaccinate response teams under IND conditions.
In outbreak, offer vaccine under IND, consistent with CDC guidelines, plus selective immunization for military forces deemed at risk, according to military situation.
9. Consider prepositioning some vaccine and VIG OCONUS
? DoD vaccine requirement from 300K to 12M doses
Accelerate production of cell-culture vaccine and VIG
Consider pre-outbreak vaccination of workers at high risk with IND vaccine, in parallel with evolving CDC guidelines for comparable civilian categories (e.g., health-care workers, laboratory workers, civil support teams).
Evaluate benefits and risks of resuming universal smallpox vaccination of military personnel:
upon FDA licensure?
sooner?
10. Points of Discussion Rational distinctions between military personnel & civilian populace:
How special are military personnel ?
Ally how closely with civilian policies ?
Contagion: Smallpox is different
How aggressively should we pursue pre-outbreak vaccination in 2002 ?
Just response teams ?
How completely should we isolate vaccinees ?
What have we failed to consider ?
11. Planning Domains Threat: Assessment, surveillance, sampling
Military Operations: Crowd control, restrictions on movement
Supply: Dryvax, VIG, needles, cidofovir, cell-culture vaccine
Regulatory: INDs (multiple), education products, waive consent ?
Policy Implications:
Vis-�-vis civilian policies, international allies
Mandatory before outbreak, for "routine" situations ?
Mandatory before outbreak, deployment or operations ?
Mandatory after outbreak, without international travel ?
Mandatory after outbreak, with international travel ?
Clinical Care: Scarification, vaccination exemptions, adverse event management, vaccinee isolation, worker safety. Variola -- Patient evac/movement, decontamination, patient isolation, patient care (pain, etc), clinical sampling.
Education, Training, Communication
Vaccination: Who first ? Where first ?
Plasma Donors for VIG-IV: Recruiting donors, processing donors
Response to Outbreak: Epidemiologic, vaccination, treatment