Download
1 / 29
380 likes | 758 Views
Dietary Reference Intakes . What Nutritionists and Other Health Professionals Need to Know. Dietary Reference Intakes. examples: vitamin C and calcium. DRI Process. North American Initiative Institute of Medicine and Health Canada Each panel has at least 1 Canadian

E N D
Dietary Reference Intakes What Nutritionists and Other Health Professionals Need to Know
Dietary Reference Intakes • examples: vitamin C and calcium
DRI Process • North American Initiative • Institute of Medicine and Health Canada • Each panel has at least 1 Canadian • Canadians review draft document • Intended to replace 1989 RDAs and 1990 RNIs • Not just traditional nutrients
Components of the DRIs • Four values instead of one • These are: • EAR: Estimated Average Requirement • RDA: Recommended Dietary Allowance • AI: Adequate Intake • UL: Tolerable Upper Intake Level • How derived? How Interpreted?
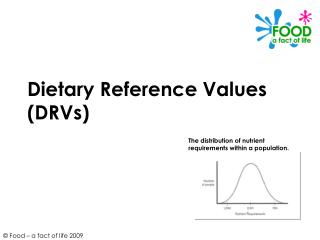
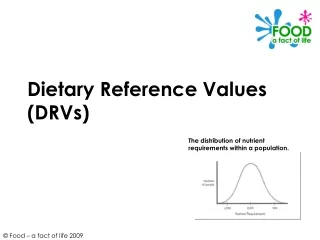
EAR and RDA values • EAR • obtain scientific data to estimate the average requirement for a nutrient • Add 2 SD to this value so that 98% of popn has their requirement met • Resulting value is RDA • RDA = EAR + 2 SD
EAR and RDA (cont) • In preceding diagram, EAR set at 45 units • RDA is 63 units • Therefore, RDA = EAR +2(9) • MOST nutrients: RDA = EAR + 2(10%) • Can be written as RDA = EAR x 1.2
Use of DRIs • Apply to healthy people • RDA is generous: covers 98% of popn • Compare to usual (average) intake, not intake on any given day • RDA is goal for an individual • EAR used to assess groups
Nutrients Without an EAR – Do Not Have RDA • Need scientific studies to determine EAR • Nutrients without EAR do not have an RDA • Instead: given an AI • Used as goal for individual (~ RDA) • We cannot assess groups using an AI • Calcium, Vitamin D, Fluoride, Biotin, Pantothenic acid (and all infant values)
Nutrients Recognized as Toxic • UL value assigned to many nutrients • Often based on case reports, not studies • Value at UL has no risk • Risk increases with higher intake • sustained intake not a single dose (except Mg)
Vitamin C Has an EAR Has an RDA Has a UL Important yet not much is known Calcium No EAR Has an AI Has a UL Important but controversial Examples to Illustrate DRIs
Vitamin C • Many functions: • Enzyme cofactor for collagen synthesis • Involved in synthesis of hormones, neurotransmittors • Now recognized as important anti-oxidant • Increases Fe absorption • In cells plasma urine excretion • in specialized tissues: WBCs
EAR and RDA for Vitamin C • EAR = 75 mg for adult men 60 mg for women • Based on following study: • 7 healthy men lived in for 6 months • Fed low C diet (5 mg/d) until depleted • Given graded doses until steady state reached • Measured serum, neutrophil, and urine ascorbate
EAR for Vitamin C • At 100 mg, neutrophils were saturated with acorbate in 4/7 subjects, but urine excretion was high (25% of dose) • At 60 mg, neutrophils were not quite saturated, but urine excretion 0 % • Panel chose value between 60 and 100 => 75 mg, as level of “adequate” vitamin C levels in WBCs
How do we assess Vitamin C adequacy? • Find usual intake of vitamin C in population • The percent of the pop’n whose intakes are below EAR = % at risk for inadequacy • In following figure, North Americans have some risk of inadequacy: • ~ 10-20% ingesting too little
Vitamin C RDA • Use RDA as a goal for an individual • RDA = EAR + 2 SD • Men: RDA = 75 + 2(7.5) = 90 mg • Women: RDA = 60 + 2 (6) = 75 mg (rounded) • Smokers – need more • Add 35 mg to RDA
Vitamin Toxicity • Many “problems” attributed to vitamin C • Excess oxalate, uric prodn kidney stones • Pro-oxidant • Fe absorption iron overload • B12 • Rebound scurvy • DRI panel found no evidence for anything except GI disturbances (osmotic diarrhea)
UL for Vitamin C • Uncontrolled cases and several controlled studies show that some people get GI disturbances at >3 g • 3 g = LOAEL • Since UL is set so no risk of adverse effects, Then UL = 3/1.5 = 2 g (~ NOAEL)
Calcium • Panel chose “desirable daily calcium retention” as criterion for setting AI • Retention is classically measured as calcium balance (Intake – Losses); assume what is retained is in bones • Now, can directly measure bone mineral content BMC ~ mineral in bone
AI for Calcium • Age 19-30: retain 10-50 mg/day, estimate 957 mg intake from old balance studies • “Judge” 1000 mg to be appropriate • At older ages (50+): clinical trial data shows less bone loss at intakes > 1000 mg • Account for less absorption at 50+ • Value set at 1200 mg
UL for Calcium • Whiting and Wood compiled case reports of “milk-alkali syndrome” in 1995 (NR ’97) • Other problems of excess Ca = kidney stones, iron absorption, Zn retention • LOAEL = 5 g (in otherwise healthy) • UL = 5g/2 = 2.5 g