Download

1 / 33
330 likes | 522 Views
CML SPIRIT 3 Steve O ’ Brien Northern Institute for Cancer Research Newcastle University Medical School. Newcastle, March 2013. Thank you!. www.spirit-cml.org. Imatinib vs Dasatinib. Acknowledgements. SPIRIT 1 study design. Randomised open label study 3 treatment arms

E N D
CML SPIRIT 3 Steve O’Brien Northern Institute for Cancer Research Newcastle University Medical School Newcastle, March 2013
Thank you! www.spirit-cml.org Imatinib vs Dasatinib
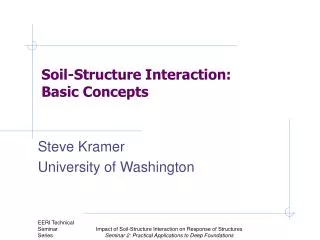
SPIRIT 1 study design Randomised open label study 3 treatment arms Arm A: 400mg daily imatinib Arm B: 800mg daily imatinib Arm C: 400mg daily imatinib plus 180mg weekly PEGinterferona Primary endpoint To compare overall survival in the three arms at 5 years N=259 Arm A: Imatinib400 Chronic phase CML Within 3 months of diagnosis R Arm B: Imatinib800 Arm C: Imatinib400 + IFN
Imatinib: SPIRIT 1 and trials like it • 10 year survival >85% • More imatinib isn’t any better • Adding interferon… • Seems better (France) • Not so sure (Germany) • No difference in survival • UK doesn’t like interferon
SPIRIT in France: IFN stays the distance Preudhomme al., New England Journal of Medicine, 2010
SPIRIT 2: Study Design Arm A Imatinib400 R Chronic phase CML within 3 months of diagnosis Arm B Dasatinib100 Randomised open label study Primary endpoint: 5 year EFS Secondary: cyto, molec response, tox
810 of 810 patients recruited! 246 since last year 172 sites currently participating 136 sites have recruited 41 more than last year not quite…
So where are we now? • Most CML patients are fine • There are more and more… • Not much difference between TKIs? • Apart from cost and perhaps side effects • Use wisely/selectively • Imatinib off patent 2016 • We really need to figure out how to reduce and/or stop treatment for a lot more patients
CML in 2013 Efficacy Side effects QoL Greatest benefit (cost)
SPIRIT 3A Phase III Randomized Trial to Evaluate the Most Effective Way to Use Imatinib, Nilotinib, and Ponatinib in Newly Diagnosed Chronic Phase Chronic Myeloid LeukemiaUK National Cancer Research Institute CML Working GroupProf Stephen O’Brien, Newcastle University
Stage 1 Compare first line intervention Randomised Stage 2 Identify partial responders early Switch Stage 3 Identify ‘best’ responders later Reduce/stop Primary endpoint: MR3 (MMR) at 3 years Secondary: sustained MR3 CMR on reduced dose/stop (no more bone marrows!) EFS, PFS, OS Health Economics, QoL SPIRIT 3 Newly diagnosed
Imatinib Stage 1 Compare first line intervention Randomised R Nilotinib 1000 patients Stage 1: up front randomisation
Overall Survival (OS)BCR-ABL (IS) at 3 months ≤1% vs. 1-10% vs. >10% ≤1% 1-10% >10% BCR-ABL (IS) n 5Y-OS ≤1% 218 97% 1-10% 283 94% >10% 191 87% p-value n.s. 0.012 Hanfstein et al. Leukemia. 2012 Mar 26. doi: 10.1038/leu.2012.85. [Epub ahead of print]
Imatinib >10% PCR ~25% patients Stage 2 Identify partial responders early Switch Stay in SPIRIT 3 Switch to ponatinib Nilotinib >10% PCR ~10% patients Stage 2: nilotinib/ponatinib? for >10% @ 3 months
Comparison A Nilotinib Nilotinib Ponatinib B Ponatinib Imatinib Imatinib
Primary objective To determine whether, in terms of major molecular response (MMR, MR3) at three years, first-line treatment with imatinib is non inferior to first-line treatment with nilotinib when patients on either treatment who are not responding optimally at 3 and 12 months are ‘rescued’ with ponatinib.
Primary endpoint • Rate of MR3 at 3 years in groups A & B • Is group A non-inferior to group B?
(DESTINY pilot) Minimum of 3 years:Halve dose if MMR for 1 year Minimum of 4 years: Stop if remain in MMR Stage 3 Identify ‘best’ responders later Reduce/stop Primary endpoint: MR3 (MMR) at 3 years Secondary: sustained MR3 CMR on reduced dose/stop (no bone marrows) EFS, PFS, OS Health Economics, QoL How much is enough?
Stage 1 Compare first line intervention Randomised Stage 2 Identify partial responders early Switch Stage 3 Identify ‘best’ responders later Reduce/stop SPIRIT 3 2013
Patients’ views • What do you think about SPIRIT 3? • Home care • Keeping you informed
SPIRIT 3 arrangements • Design: NCRI CML Working Group • Sponsor: Newcastle Hospitals NHS Trust • Funder: Ariad • NCRI badged, CTAAC approved 2012 • Trial management: Newcastle CTU • Governance: TMG, TSC, DMEC • Drug supply: • Imatinib & nilotinib – NHS, home delivery, VAT • Ponatinib – free of charge for 10 years, home delivery
SPIRIT 3 practicalities • No more marrows • Unless you want/need to • PCR essential, especially 3 months and stage 3 • Check BP regularly, CV risk • Home delivery, no hospital pharmacy stock • Pharmacy clinical check • Biobanking material • Blood and mouthwash • More direct patient & investigator involvement • Web, apps, meetings
SPIRIT 3 translational research • UK wide collaboration • Newcastle, Liverpool, Glasgow, Edinburgh, Imperial, Kings • Comprehensive biobanking • Leukaemia, ‘normal’ tissue • Factors predicting response, outcome, ability to reduce/stop • Stem cell biology, NGS (WGS, ES), PCR, TKD mutations, PK
Stage 1 Compare first line intervention Randomised Stage 2 Identify partial responders early Switch Stage 3 Identify ‘best’ responders later Reduce/stop Primary endpoint: MR3 (MMR) at 3 years Secondary: sustained MR3 CMR on reduced dose/stop (no more bone marrows!) EFS, PFS, OS Health Economics, QoL SPIRIT 3 Newly diagnosed
Questions? Thanks for listening
CML SPIRIT 3 Steve O’Brien Northern Institute for Cancer Research Newcastle University Medical School Newcastle, March 2013