Download
1 / 30
320 likes | 701 Views
Neonatal Physiology and Anesthesia. Elena Brasoveanu, MD Boston University March 2, 2006. Pediatric Anesthesia. Origin in the 1930’s at Toronto Hospital for Sick Children when Robson described techniques only for children

E N D
Neonatal Physiology and Anesthesia Elena Brasoveanu, MD Boston University March 2, 2006
Pediatric Anesthesia • Origin in the 1930’s at Toronto Hospital for Sick Children when Robson described techniques only for children • Recognized subspecialty starting with 1946 when Robert Smith became director of anesthesia at Boston Children’s Hospital • Now, approximately 49 fellowship programs
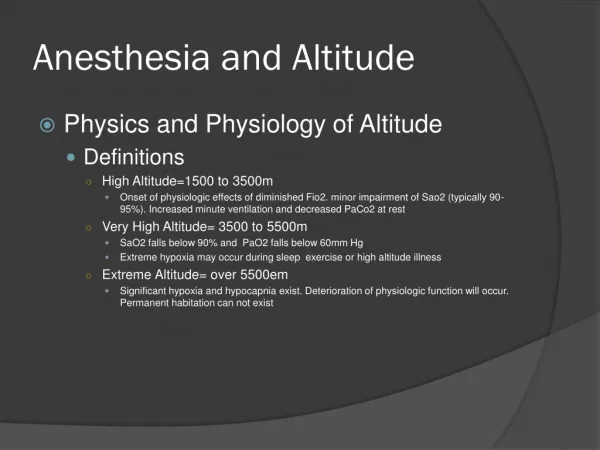
Aspects of the Neonatal Physiology • The neonatal oxygen consumption is approximately 6 ml/kg/min versus 3 ml/kg/min in the adult • Even under normal circumstances the immature cardiac and respiratory systems must function near maximum to support this metabolic demand.
Respiratory Physiology • The respiratory system is not fully developed at birth and continues through early childhood. • Airways fully developed at 16 wks of gestation • Alveolarize at 24-28 wks with complete maturation at 8 - 10 y.o.
Respiratory Physiology (cont’d) • Increasing respiratory rate rather than tidal volume is more efficient to increase alveolar ventilation • The diaphragm is the primary respiratory muscle – has fewer high-oxidative muscle fibers and is less resistant to fatigue than the adult diaphragm
Respiratory Physiology (cont’d) • Awake FRC is similar, when normalized to body weight, to that of an adult • FRC declines during anesthesia and combined with hypoventilation and increased consumption causes a rapid desaturation
Respiratory Physiology (cont’d) • Central apnea- self limited in newborns, approximately 5 seconds • Apnea of prematurity – 20 seconds or associated with desaturation episodes and bradycardia • Resolves at 50- 55 weeks gestational age.
Respiratory Physiology (cont’d) • Chest wall development • Ribs oriented parallel and unable to increase the thoracic volume during inspiration • At 2 y.o., associated with standing and walking, ribs are oriented oblique • Cartilaginous structure with inward movement during inspiration
Developmental Changes of the Rib Cage Reproduced from - R. S. Litman: Pediatric Anesthesia – The Requisites in Anesthesiology, Elsevier Mosby 2004
Respiratory Physiology (cont’d) • Production of surfactant begins at 23 – 24 wks of gestation and reaches maturation after 35 wks of gestation • Decreased surfactant production in preterm babies decreases the compliance – risk for respiratory distress syndrome, bronchopulmonary dysplasia and pulmonary hypertension
Respiratory Physiology (cont’d) • Respiratory Distress Syndrome • Perinatal asphyxia • Maternal diabetes • Multiple pregnancies • Cesarean section delivery
Respiratory Physiology (cont’d) • Respiratory Distress Syndrome – treatment • Steroids to the mother • Surfactant intratracheally • Protective strategies for lung ventilation
Cardiovascular Physiology • Fetal circulation – high pulmonary vascular resistance, low systemic resistance (placenta) and right to left shunt via PFO and DA. • Aeration of the lungs – decrease pulmonary vascular resistance, mediated by NO, increase systemic resistance by placenta removal
Fetal Circulation Reproduced from - R. S. Litman: Pediatric Anesthesia – The Requisites in Anesthesiology, Elsevier Mosby 2004
Cardiovascular Physiology (cont’d) • The neonatal pulmonary circulation is very reactive • Hypoxemia, hypercarbia, acidosis can cause pulmonary vasoconstriction and opening of the DA.
Cardiovascular Physiology (cont’d) • Neonatal myocardium contains immature contractile elements and is less compliant than the adult myocardium • Limited increase in CO by volume load in a normovolemic newborn • CO rate dependent
Cardiovascular Physiology (cont’d) • Adrenergic receptors mature at birth but sympathetic innervation is incomplete • To meet increased metabolic demand, the CO relative to body weight is twice that of the adult. • CO is 350ml/kg/min in newborns, 150 ml/kg/min at 2 months of age • The baroreflex activity is impaired and a 10% reduction in blood volume will cause a 15-30% decrease in MAP
Cardiovascular Physiology (cont’d) • The electrocardiogram shows an axis oriented to the right due to right dominance.
Newborn EKG Reproduced from - R. S. Litman: Pediatric Anesthesia – The Requisites in Anesthesiology, Elsevier Mosby 2004
Open Sutures of the Newborn Cranium Reproduced from - R. S. Litman: Pediatric Anesthesia – The Requisites in Anesthesiology, Elsevier Mosby 2004
Central Nervous System • IVH occurs in 40 to 50% of premature infants and is a major cause of neonatal morbidity and mortality • At the level of germinal matrix • Careful anesthetic management to avoid hypercarbia, hypoxia, fluctuation in BP
Central Nervous System • Retinopathy of prematurity – abnormal growth of retinal vessels that leads to scarring and blindness • Risk factors: • Prematurity • Hyperoxia • Hypocarbia • Vitamin E deficiency • Acidemia
Thermoregulation • Enhanced heat loss due to: • relatively larger surface area, • thinner layer of insulation and • limited capability of heat production • Thermogenesis in brown fat is mediated by the sympathetic system and stimulated by norepinephrine, resulting in triglyceride hydrolysis.
Thermoregulation • The thermoregulatory range is the ambient temperature range within un unclothed subject can maintain normal body temperature • The lower limit of the thermoregulatory range is 10C for an adult, 230C and 280C for the full term and premature infant, respectively.
Fluid, Electrolyte, and Renal Physiology • Increased • total body water • extracellular fluid volume • water turnover rate • Reduced glomerular filtration rate • Obligate sodium losers
Changes in Body Composition Reproduced from - R. S. Litman: Pediatric Anesthesia – The Requisites in Anesthesiology, Elsevier Mosby 2004
Fluid, Electrolyte, and Renal Physiology • Decreased glycogen stores – prone to hypoglycemia • The term neonate requires 3 to 5mg/kg/min of glucose to maintain euglycemia • Glucose should be maintained between 35 and 125 mg/dl. • Hyperglycemia predisposes to intracranial hemorrhage
Hematologyc Physiology • At birth Hb is 19g/dL represented by HbF • Physiologic anemia of infancy – at 6 to 10 weeks of life, the HbF is replaced by HbA • There is no indication for transfusion in the absence of clinical signs of anemia • Coagulation factors are decreased at birth but normalize during the first year of life
Bibliography: • S. C. Hillier, G. Krishna, E. Brasoveanu: Neonatal Anesthesia. Seminars in Pediatric Surgery: Pediatric Anesthesia, vol 13/3, August 2004. • R. S. Litman: Pediatric Anesthesia – The Requisites in Anesthesiology, Elsevier Mosby 2004, pg3 to 18, 68 to 72. • E.K. Motoyama, P.J. Davis: Smith’s Anesthesia for Infants and Children, Elsevier Mosby 2006, pg 12 to 148.