Download
1 / 37
1.02k likes | 2.69k Views
RESPIRATORY PHYSIOLOGY DURING ANESTHESIA. Presenter – Hitesh Gupta Moderater – Dr Anil Ohri. Anesthesia - impairment in pulmonary function whether patient is breathing spontaneously or ventilated mechanically after muscle paralysis .

E N D
RESPIRATORY PHYSIOLOGY DURING ANESTHESIA Presenter – Hitesh Gupta Moderater – Dr Anil Ohri
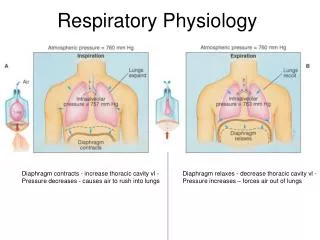
Anesthesia - impairment in pulmonary function whether patient is breathing spontaneously or ventilated mechanically after muscle paralysis. • 20% of patients may suffer from severe hypoxemia(spo2 81% for up to 5 minutes)
GA produces • Fall in FRC • Fall in lung compliance • Uneven distribution of ventilation • Increased physiological dead space • Increased P(A-a)O2
FRC reduced by 0.8 to 1.0 L - changing body position from upright to supine another 0.4- to 0.5-L - when anesthesia is given. • Muscle paralysis and mechanical ventilation cause no further decrease in FRC. • average reduction corresponds to around 20% of awake FRC
Cranial shift of diaphragm and a decrease in transverse diameter of the thorax contribute to lowered functional residual capacity (FRC). • Decreased ventilated volume (i.e. in atelectasis and airway closure ) is a possible cause of reduced lung compliance (CL). • Decreased airway dimension by the lowered FRC should contribute to increased airway resistance (Raw).
Causes of reduced FRC • General anesthesia: • due to loss of respiratory muscle tone, which shifts the balance between the elastic recoil force of the lung and the outward force of the chest wall to a lower chest and lung volume. • Maintenance of muscle tone(ketamine anesthesia) does not reduce FRC • Supine Position: • FRC decreases by 0.8-1.0L • Diaphragm cephalad displacement
.Immobility, excessiveintravenous fluid administration: • Dependent areas below the heart (zone3-4) are susceptible to edema • this will happen after being immobile (5 hour or more) in supine position with excess volume administration
.Surgical position: • Supine : FRC • Trendelenburg: FRC • Steep trendelenburg: FRC • Lateral decubitus : FRC in dependent lung and FRC in un dependent lung (overall FRC ) • Lithotomy : FRC more than supine • Prone : FRC Prone> lateral decubitus > supine > lithotomy> trendelenburg> steep trendelenburg
Ventilation pattern: • Rapid shallow breathing occurs due to reduced compliance - FRC • This can be prevented by • Periodic large mechanical inspiration • Spontaneous sigh • Peep
. Decreased removal of secretion: Increasing viscosity & slowing mucocilliary clearance • Tracheal tube (low or high pressure cuffs any place in trachea) • High FiO2 • Low moisture • Low temperature • Halogenated anesthetics
Compliance and Resistance of the Respiratory System • Static compliance(lungs and chest wall) is reduced – from 95 to 60 mL/cm H2O during anesthesia • static lung compliance- 187 mL/cm H2O awake to 149 mL/cm H2O during anesthesia • Resistance( total respiratory system and lungs)increases both spontaneous breathing and mechanical ventilation • increased lung resistance reflects reduced FRC during anesthesia
Causes of decreased lung compliance • Atelectasis • 15% to 20% of lung is collapsed at the base of lung during uneventful anesthesia. • thoracic surgery and cardiopulmonary bypass > 50% of the lung can be collapsed. • decreases towards apex of lung • increases with BMI but is independent of age • COPD patients show less atelectasis • Risk factors: High FiO2 Low V/Q ratio Longer time exposure of high FiO2 to low V/Q
ZONE A – ventilation > perfusion resulting in dead space like effect • ZONE B – perfusion > ventilation leading to low Va/Q and caused impaired oxygenation of blood due to intermittent airway closure • ZONE C – there is complete cessation of ventilation (atelectasis) but still perfusion is there (shunt)
Prevention of atelectasis • Positive end expiratory pressure (PEEP) • Application of 10 cm water PEEP can open collapsed lung but it recollapses on cessation of peep • Gen PEEP of 10 cm H2O squeezes perfusion to lower lung • Selective application of PEEP to lower lung might lead to redistribution to upper lung
Maintenance of muscle tone • Anesthetic that allows maintaince of respiratory muscle tone will prevent atelectasis e.gketamine • Pacing of diaphragm through phrenic nerve stimulation prevents atelectasis ,but is too complicated
Recruitment maneuvers • Sigh maneuver • Double VT airway pressure of 30 cm of H2O decrease atelectasis by 50 % of initial size for complete reopening 40 cm of H2O is req.
Prevention of atelectasis • VC maneuver Vital capacity maneuveris the volume inflated to the maximum breath by the awake subject before anesthesia. Inflation of lungs to +40 cm H2O maintained for no more then 7 to 8 sec re expand all previously collapsed lung tissue
Prevention of atelectasis • Minimising gas resorption • 100% O2 - collapse reappears faster but using 40% O2 in nitrogen, atelectasis appears slowly • Avoidance of preoxygenation procedure (ventilation with 30% O2) eliminates atelectasis formation during induction and subsequent anesthesia • CPAP of 10 cm H2O can prevent atelectasis even with 100 % O2
Prevention of atelectasis • Postanesthetic oxygenation • Postanesthetic oxygenation (100% O2) 10 minutes before termination of anesthesia together with a VC maneuver at the end of anesthesia will not protect against atelectasis at the end of anesthesia • VC maneuver followed by a low O2 concentration, 40% keeps the lung open after recruitment until end of anesthesia.
Airway Resistance • Increase airway resistance, leads to airway collapse • Factors: • Decreases in FRC • ETT • Upper and lower airway passages • External anesthesia apparatus
Uneven distribution of ventilation • Uneven distribution • Right > left • Nondependent > dependent • PEEP increases dependent lung ventilation
Distribution of Lung Blood Flow(Perfusion) • Uneven distribution Base> apex • successive increase in perfusion down the lung, from the ventral to the dorsal aspect. • PEEP impede venous return to the right heart and therefore reduce cardiac output. • PEEP causes a redistribution of blood flow toward dependent lung regions.By this upper lung regions may be poorly perfused,causing a dead space–like effect.
V/Q ratios • V/Q ratio: 0.8 • Shunt: V/Q ratio =0, perfusion only • Dead space: V/Q ratio =infinity, ventilation only • Perfusion increases at a greater rate than ventilation • Apical area: higher V/Q ratio • Basal area: lower V/Q ratio (shunt)
during anesthesia increased VA /Q mismatch increased Venous admixture (approx 10% cardiac output). increased alveolar dead space
Hypoxic Pulmonary Vasoconstriction • Normally PaO2 decrease will cause HPV • inhaled anesthetics inhibit HPV . Aggravate an existing V/Q mismatch • no such effect seen with intravenous anesthetics (barbiturates) • isoflurane and halothane depress the HPV response by 50% at 2 MAC • Direct: nitroprusside ,NTG, Isoproterenol ,inhaled anesthetics, hypocapnia • Indirect: MS , fluid overload, high fio2 , hypothermia ,emboli, vasoactive drugs, lung disease
Effect of depth of anesthesia on respiratory drive • Inhaled anaesthetics and barbiturates reduce sensitivity to CO2 and the effect is dose dependent. • due to impeded function of intercoastal muscles • Anaesthesia also reduces response to hypoxia due to effect on carotid body receptors
Effect of depth of anesthesia on respiratory pattern • Less than MAC vary from excessive hyperventilation to breath holding • 1 MAC (light anesthesia) regular pattern with larger VT than normal • More deep end inspiration pause (hitch) – active and prolong expiration
Effect of depth of anesthesia on respiratory pattern • More deep (moderate) faster and more regular – shallow –no pause – Inspiration = Expiration • Deep • Narcotic- N2O : Deep and slow • Volatiles : rapid & shallow (panting) • Very deep all inhaled drugs : gasping-jerky respiration – paradoxical movement of chest-abdomen (only diaphragmatic respiration) just like airway semi obstruction or partial paralysis
Effect of depth of anesthesia on spontaneous minute ventilation • Minute ventilation decreases progressively as depth of anesthesia increases • ET CO2 increases as depth of anesthesia increases • Increase of CO2 caused by halogenated anesthetics (<1.24 MAC) enflurane > desflurane =isoflurane > sevoflurane> halothane (>1.24 MAC) enflurane = desflurane > isoflurane > sevoflurane • Ventilation response to CO2 increase is decreased • Apnea thresholdis increased
Factors That Influence RespiratoryFunction During Anesthesia • Spontaneous Breathing • FRC is reduced to the same extent during anesthesia • atelectasis occurs to almost the same extent in anesthetized spontaneously breathing subjects as during muscle paralysis.
Increased Oxygen Fraction • As Fio2 is increased, shunt is also increased • explained by attenuation of HPV response with increasing Fio2 or further development of atelectasis and shunt in lung units with low VA /Q ratios Body Position • FRC is reduced in supine position • Lateral position causes severe impairment in arterial oxygenation in some patients. • ventilation distribution was more uniform in anesthetized subjects who were in the prone position
Age • arterial oxygenation is impeded with increasing age of the patient • shunt is independent of age 23 to 69 years • There is increasing VA /Q mismatch with age • major cause of impaired gas exchange during anesthesia at ages younger than 50 years is shunt, whereas at higher ages mismatch becomes increasingly important.
Obesity • worsens the oxygenation of blood • markedly reduced FRC, which promotes airway closure to a greater extent than in a normal subject • PEEP , CPAP or near-VC inflations followed by PEEP ventilation
Preexisting Lung Disease • Smokers and patients with lung disease have severe impairment of gas exchange in the awake state as well as during anesthesia • smokers with moderate airflow limitation have less shunt, however, considerable Va /Q mismatch with a large perfusion fraction to low Va /Q regions • Reason - chronic hyperinflation which changes the mechanical behavior of the lungs and their interaction with the chest wall such that the tendency to collapse is reduced • these low Va /Q ratios can be converted over time to resorptionatelectasis.
Regional Anesthesia • extensive blocks (thoracic and lumbar segments)-inspiratory capacity is reduced by 20% and expiratory reserve volume approaches zero. • Diaphragmatic function is often spared, even in sensory block up to the cervical segments. • Arterial oxygenation and carbon dioxide elimination are well maintained
Thank you