Download
1 / 27
280 likes | 488 Views
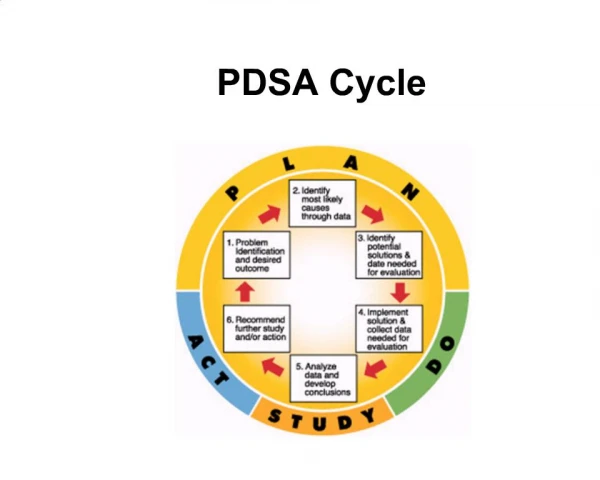
Rangel PDSA TB Didactic. TB or not TB?. AIM Statement.

E N D
Rangel PDSA TB Didactic TB or not TB?
AIM Statement • In order to improve care at the Charles Rangel Clinic, we will implement a tuberculosis screening protocol in order to identify high risk patients aged 1-11 years old who require PPD placement according to the guidelines set forth by the AAP Committee on Infectious Disease.
AIM Statement • Our goal • ≥95% of our patients will have documented screening for tuberculosis risk factors at least yearly • ≥95% of patients with documented risk factors will have a PPD placed AND read • follow those in whom treatment is warranted
Why pediatric TB is important: • 30% of global TB cases; 7% in U.S. • Age 0-4 more likely to develop active TB once infected and more vulnerable to disseminated TB • Public Health Standpoint:Pediatric TB = Sentinel Event • Worldwide, 500,000 children die annually from TB
Routine pediatric care: No more universal testing • Not cost-effective to routinely skin test healthy children without risk • Up to 85% of positive results will be FALSE positives in areas of low TB prevalence • Preferred strategy: “targeted testing” • Focuses testing children with risk factors • Screen all children for risk factor(s) • Test only if > 1 risk factor(s) present
PDSA Cycle 1:TB screening questions • To be asked once yearly at well child visits in children between the ages of 1 and 10: • Was your child or any household member born outside the United States? • Has your child or any household member traveled outside the United States? • Has your child been exposed to anyone with TB disease or a positive PPD? • Does your child spend time with anyone who has been in jail (or prison) or a shelter, uses illegal drugs, or has HIV?
Cutoff PPD values • 5mm is positive when • close contact with known or suspected contagious tuberculosis • suspicion of disease based on clinical factors, or radiologic abnormalities • 10 mm is positive when • risk for dissemination, including those younger than 4 years or those having medical conditions such as HIV diabetes renal failure or solid tumors • increased exposure such as frequent exposure to HIV infected persons, drug users, incarcerated persons, or nursing home residents • areas endemic for TB and those who have contact with adults from those areas (Asia, Middle East, Africa, Latin America) • 15 mm is positive when • 4 years of age and over without any risk factors
PDSA Cycle 2:Baseline Measures • Chart review of all well child visits on 2 consecutive Tuesdays • 19 patients were screened for tuberculosis risk factors • 8 (42%) of the patients screened had at least one risk factor • 3/8 (38%) did not have PPD placed • 2/8 (25%) had PPD placed: 1 patient did not return for the reading. 1 patient had positive read and was referred for CXR and started on INH • 1/8 (13%) had a documented negative PPD in the chart and was not retested • 2/8 (25%) could not be followed due to missing charts
All the screening questions, in one nice neat little box – oh the joys of modern medicine!!
PDSA Cycle 3: Old Projects revisited
PDSA Cycle 5 • Assessed return rate for PPD readings in January • 15 PPDs placed • 12 (80%) returned for reading in the appropriate amount of time All 12 were read as negative • 1 (7%) did not return • 2 (13%) still pending at the end of the cycle
The Rangel Clinic’s state of the art Mead Composition Book has a 0% “system shut down from 1-3am” rate!
page from 7/2007 page from 4/2008 Over the course of the year – increased messiness possibly correlating with increased activity!
PDSA Cycle 5:Keeping Track of PPD Placement • Implemented a “PPD placement note” into Eclipsys • Started by the nurse at the time of placement and kept “incomplete” • Note completed when the patient returned for PPD read • Unfortunately, this did not completely solve the issues: • Unable to filter PPD notes in Eclipsys • Difficult to keep track of outstanding PPD and results
PDSA Cycle 6:Improving Tracking • Organized with the nurses that PPD notes in Eclipsys should include the ordering MD as a co-signer for the note. • MD and nurse share the responsibility of following up on results • Talked to Eclipsys administrators to create a filter for patients who have PPDs placed in a given time
PDSA Cycle 6:Reviewing Positive PPDs • Review of positive PPDs over 3 years (2005-2008) • 6 patients with positive PPDs documented • 4 of these patients had charts available for review • 2/4 (50%) had documented CXR and INH treatment
PDSA Cycle 7:Progress of PPD Tracking • Chart review January 30-February 17 • 94% of PPDs placed had a PPD placement note in Eclipsys • 70% returned for PPD read, 100% negative • 17% of these were co-signed to a physician • When a note is updated in Eclipsys, all co-sign data gets erased and must be reassigned • Our head nurse reminded staff to reassign a co-signer each time the note was accessed
PDSA Cycle 7Reassess TB Screening • Chart review of patients presenting on 1 day of clinic • 75% of the charts had documentation of TB screening during a WCC over the past year • 100% who screened positive had PPDs placed • 100% of the patients who returned for their read were read as negative
PDSA Cycle 8:Positive PPD requirements • 100% of PPDs placed were read as negative • Induration >10mm was always read as postive. • Unclear what to do with induration >5mm. • Nurses and physicians re-educated about definition of positive PPD • Red Bood guidelines posted in nursing office
The Future of TB at Rangel • TB screening is sustainable, as there is a prompt within the Eclipsys ambulatory note • Once screened, placing a PPD is also simple • Issues still lie with improving return rate for PPD reads • Reminder phone calls to families regarding visit • Implementation of Televox system
PDSA Cycle 3:Old Projects Revisited • 25 charts (8/07-9/07) coded “WCC” for ages 6 months to 4 years were reviewed for documentation of dental screening and and lead risk. • 5/25 had documentation of dental screening (20%) • 8/25 had documentation of lead risk factors (32%) • 3/25 had documentation of both (12%)
PDSA Cycle 3:Old Projects Revisited • A presentation reviewing our previous projects was given on each clinic day • To improve documentation rates utilized Eclipsys: • “Dental” check box should be added to the Eclypsis note with a free text box • The lead risk factors check box, which existed in the “Social” portion of the note should be in its own separate drop box.