Download
1 / 15
150 likes | 699 Views
Cheshire and Merseyside Rehabilitation Network. Network Establishment. 2 year project – completed Jun 13 9 Hyper- acute Rehabilitation beds – for patients with the most complex nursing and medical needs 20 Supportive Rehabilitation beds within the Complex Rehabilitation Unit

E N D
Network Establishment 2 year project – completed Jun 13 9 Hyper- acute Rehabilitation beds – for patients with the most complex nursing and medical needs 20 Supportive Rehabilitation beds within the Complex Rehabilitation Unit 35 Spoke Unit beds across Elyn lodge and Broadgreen 16 ABI Rehabilitation beds within extended rehab unit (Merseyside) 4 Rehabilitation Consultants in post 9 Specialist Professional groups working across the pathway 1 Therapy Out-patient Team - St Helens Spoke 1 Specialist Complex Rehabilitation Community Team – St Helens, Halton and Knowsley
Objective • To ensure that the network collects robust data, which records treatment outcomes and quality of life of service users during and following care and treatment from the network Why? • The ‘usual’ NHS definition of success of treatment is a clinical definition and is incomplete
Network Standards and KPI’s 49 Key Performance Indicators including: 1 UKROC outcome measure 3PROMS/PREMS 17 Quality and performance Indicators 23 Standards drawn from nationally recognised bodies e.g. British Society for Rehabilitative Medicine to demonstrate evidence of compliance 11Service Specs. e.g. Neuropsychiatry, Neuro and Clinical Psychology, Bed Management Service, Support Wellness and Advice Service & Podiatry
Scale of Pain Intensity Tool (SPIN) 1 Does the service show signs of pain 2How severe is the pain? – measured against SPIN scale 3 Does the service user understand the SPIN scale? Three options (can mix and match) Evaluate pain daily and reduce/ control Refer to Speech and Language therapy for communication support Refer to neuropsychology for assessment/ongoing care
Depression Intensity Circles (DISC) 1 Does the service user complain of sadness or depression 2How severe is the depression? – measured against DISC scale 3 Does the service user understand the DISC scale?
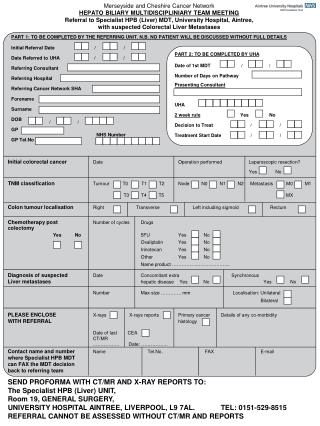
To Administrator, please ensure all 3 questions are completed, including NAME and DATE The DISCs Screen. Patient Name…………………………………. Date…………………….. Comments: e.g. “I feel sad, but not depressed” – explain.. • 1. Yale question: • Do you often feel • sad or depressed? Yes No 2. The DISCs • Instructions for administration: • Say to the patient: • This is a scale to measure depression • Please point to each of the circles in turn to make sure that you can see them all. • [Continue only if satisfactorily accomplished] • The grey circles show how depressed you feel. • [Indicate the clear circle at the bottom] • The bottom circle shows no depression. • [Indicate the fully shaded circle at the top] • The top circle shows depression as bad as it can be. • [Pointing at each circle in ascending order] • As you go from the bottom circle to the top, you can see that depression is becoming more and more severe. Ask; How depressed do you feel today? Most severe depression Yes No Not sure No depression If not sure, refer for Full screen 4. Summary of screen Depressed – refer to Integrated care pathway Not depressed – re screen in 4 weeks Date of re-screen ……………… 3. To the administrator: In your opinion, does the patient understand this scale? Comments: 5. Re-screen Depressed – refer to Integrated care pathway Not depressed – pathway closed Date pathway closed ………………
Case Studies Patient A - 43yr old man - pedestrian vs car with poly-trauma and multiple thoracic fractures. History of substance misuse. Admitted from Major Trauma Centre to the Complex Rehabilitation Unit for 6 weeks. Discharged independently mobile and self caring, complex discharge planning due to housing issues. Patient and family referred to support groups and voluntary agencies prior to discharge.
Case Studies Patient B - 63 yr old man with poly-trauma and orthopaedic injuries following attempted suicide. Admitted from Major Trauma Centre, transferred within 3 days of acceptance to pathway to the Complex Rehab Unit for 9 weeks Supportive Rehabilitation. Discharged home mobile and self caring with IV therapy input whilst awaiting further orthopaedic surgery.
Opportunities Realised • Improved standards of clinical practice by working closely with service users • Established Neuro and Clinical Psychology and welfare services – in and out of hospital • Developed good working relationships- between key workers, MDT, rehab consultants, trauma staff. • Single Point of Access - effective in reducing times to access beds • Improved outcomes - 55% of discharges have gone directly home. • Development of a Centralised Database to record outcomes
Challenges Recruitment Delays Spoke Unit Access for Cheshire Patients Change in Commissioning Landscape Rehab tariff Social care - Vol. of staff/time to recruit - Commencement of BroadgreenSpoke Unit - Gap in provision - Delayed implementation of outstanding elements of pathway and ongoing - Introduction April 2014 - Limited involvement in pathway
Future Developments • Implementation of vocational and educational rehabilitation network • Network Social Work Provision • Implementation of Rehabilitation Competencies for all senior Network professionals • Specialist Complex Community Rehabilitation Service - Liverpool and Sefton locality • Therapy Out-patient Service - Broadgreen • Patient Experience Survey • Rehab Network Service Evaluation
Research and Evaluation • Evaluation - An 18 month research programme to support the evaluation of the whole rehabilitation pathway has commenced this includes: Patient experience • Outcomes – clinical and lifestyle • Evaluation of Key worker role • Evaluation of pathway model • Research – A consultant-led Clinical Research Programme is currently under development