Download
1 / 16
160 likes | 286 Views
Dr. Shay Keating The National Drug Treatment Centre. Management of Hepatitis C in the Community – one man’s journey!!!. Who am I?. A doctor The Medical Officer in the National Drug Treatment Centre (NDTC) Associate Specialist in Sexual Health and HIV – St. James’s hospital

E N D
Dr. Shay Keating The National Drug Treatment Centre Management of Hepatitis C in the Community – one man’s journey!!!
Who am I? • A doctor • The Medical Officer in the National Drug Treatment Centre (NDTC) • Associate Specialist in Sexual Health and HIV – St. James’s hospital • But mostly – I’m the ‘who the *?#@ is he?’
My journey in HCV care • It began in 1990s in the addiction services – the then ERHA – now the HSE • Very little focus on hepatitis C • Poor knowledge among the service users – ‘at least I don’t have HIV’ • Very poor information available
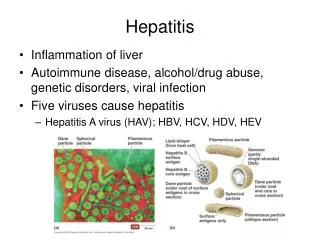
Management of HCV - What could we do in 1990s? • Refer for specialist review • Facilitate illicit drug and alcohol cessation • Optimise social support • Offer advise on minimising the risk of transmission to others • Provide further virological testing where appropriate • Immunise against hepatitis A and B • Provide information
IVDU – Irish context (approximates) IVDU in Dublin ~14000 70% HCV antibody positive ~10000 70% of those HCV RNA detected ~70000 50% genotype 1 50% ‘non 1’, mainly 3
Treating HCV Positive Drug Users in 1990s • Many drug users were socially marginalised with poor access to healthcare • Many were unaware of the dangers of HCV infection – this was improving • Many too unstable – actively using illicit drugs or alcohol • Non attendance at appointments was a significant problem in referral for specialist hepatology/ID advice – hugely frustrating for hepatology/ID, for primary care and addiction services • Adherence to treatment was often poor – SIDE EFFECTS!!! • Relapse into active addiction
Strategies to facilitate HCV treatment in IVDU • Directly observed therapy (DOT) • DOT in IVDU context refers to treatment delivery in same location where they receive their opiate replacement therapy • DOT has been shown to facilitate treatment adherence in IVDU • Drug users might miss OPD appointments but will rarely miss the drug treatment clinic and opiate substitute medication • Used for TB treatment – Salomon et al., 1997 • Used for HAART in HIV/AIDS – Sorensen et al., 1998, Clarke et al., 2000. • General practice engagement in ‘shared care’ approach • Development of HCV liaison nurse specialist positions
The National Drug Treatment Centre • The Natonal Drug Treatment Centre (formerly the DTCB) is a Specialised Addiction Centre in Dublin and the largest Drug Treatment facility in Ireland • Currently approximately 550 attendees, 80% of whom are HCV positive – many with psychiatric co-morbidities • Of those not co-infected with HIV, 70% are HCV RNA positive • Approximately 50% genotype 1 and 50% genotype 3
On-site HCV Treatment at the NDTC • In 2003, I introduced a HCV treatment pilot study with DOT into the NDTC • Rationale: ‘To treat the patients with hepatitis C in the same location in which they receive their methadone with a view to retaining the patients in treatment’ • Regular medical review – Liaison with Professor Colm Bergin, Infectious Diseases Consultant, St. James's Hospital • Regular psychiatric review
Pilot Study • Not to show that the treatment works But • A proof of concept – that patient retention in treatment can be improved if therapy is initiated in a specialist drug treatment setting with directly observed therapy and with appropriate medical and psychiatric support on site.
On-site HCV Treatment ‘Pilot Study’ • Pilot study of nine patients – 6m/3f • All HCV RNA positive genotype ‘non 1’ mono-infected – HIV and HBV negative • 8 were genotype 3, 1 was genotype 2 • Liver biopsies not performed • Stable re. drugs/alcohol for minimum of 6 months • Guaranteed contraception
Treatment endpoints • Primary • Efficacy of treatment – SVR 24 weeks post treatment cessation • Retention in treatment • Secondary • Management of medical and psychiatric complications on-site with continued drug stability
On-site HCV Treatment ‘Pilot Study’ • HCV treatment initiated at NDTC • HCV treatment team – me!, a nurse, a psychiatric registra and a counsellor • Peginterferon injection given weekly by the nurse and ribavirin was dispensed weekly on site
Pilot Study Findings • 8 of 9 - finished programme (89% retention in treatment) • 8 of 9 had an SVR (efficacy is comparable to hospital based setting) • 5 of 9 - haematological difficulties • 3 of 9 - significant depressive symptoms • 3 of 9 relapsed briefly into active addiction
Follow-up to pilot study • In 2005, the programme was extended to include HCV genotype 1 • Pathway for liver biopsy established in St. James's • Facilitated by I.D. Department/Prof Colm Bergin and Radiology in St. James's hospital
Summary • Hepatitis C is one of the treatment successes of modern medicine • Many patients have a good chance of a cure with the therapies available today • Illicit drug use is still the commonest means of contracting HCV in the developed world • Treatment delivery needs to take the subculture of illicit drug use into consideration