Download
1 / 19
200 likes | 386 Views
The effects of investing in thoracic surgery on lung cancer resection rates. David Waller , Kelvin Lau Sri Rathinam Glenfield Hospital, Leicester, UK Mick Peake UK National Lung Cancer Audit Programme. Lung cancer in UK is under treated.

E N D
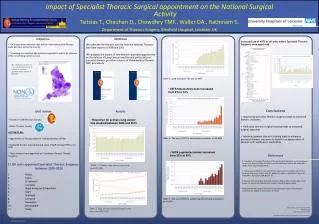
The effects of investing in thoracic surgery on lung cancer resection rates David Waller , Kelvin Lau Sri Rathinam Glenfield Hospital, Leicester, UK Mick PeakeUK National Lung Cancer Audit Programme
There is a wide variation in lung cancer surgery in England 5.2% – 10.1% 10.9% – 13.2% 13.6% – 14.5% 14.6% – 16.5% 16.9% – 31.8%
The UK National Lung Cancer Audit 2008 results • 33 English Cancer Networks, comprising 174 Hospital Trusts • 18% Trusts had Thoracic Surgical centres • 58% Trusts had less than 2 Pure Thoracic Surgeons • In 2008, 15,774 cases of confirmed lung cancer • 14.2% underwent resection
The workforce data Currently in England • 58 Pure Thoracic Surgeons • 63 Cardiothoracic Surgeons • 114 Pure Cardiac Surgeons Data from Centre for Workforce Intelligence 2010
We found from relating audit data to manpower levels that … • Resection rates are higher in centres who treat more cases • Resection rates are higher in patients first seen in base rather than in referring centres • Resection rates are higher in centres with 2 or more specialist thoracic surgeons • Resection rates are higher when surgeons attend preoperative MDTs • The 2008-2009 increase in resection rate was greatest in those units who employed new thoracic surgeons
Workforce implications In the Network with best resection rate 2008 3 Pure thoracic surgeons see 450 new cases lng cancer per year, each surgeon attends 1.5 MDTs per week For 15,700 cases need 107 surgeons For 170 MDTs need 113 surgeons If 63 cardiothoracic surgeons each devote half time = current total of 89 WTE
The bottom line … • England needs to recruit 25 – 30 new pure thoracic surgeons to maximize lung cancer resection by … • Increasing training numbers • Getting Cardiothoracic surgeons to specialize • Importing new thoracic surgeons
National Lung Cancer Audit: Patient numbers, 2008 England Cases Submitted 26,256 Wales Cases Submitted 2,133 Scotland Cases Submitted 4,058 Total Cases E & W Submitted 28,389 Excluded from Analysis (no date first seen) 575 SCLC 602 (14.8%) All lung cancer excluding small cell 3456 (85.2%) Included in Analysis 27,814 SCLC 2,909 (10.5%) Mesothelioma 1,405 (5.1%) All lung cancer excluding small cell (and mesothelioma) 23,500 (84.5%) Confirmed NSCLC 2467 (71.4%) Other 989 (28.6%) Confirmed NSCLC 15,744 (67.1%) Other 7,726 (32.9%)
Hypothesis the variability in Resection Rate is determined by the provision of specialist thoracic surgery Method We correlated results of the NATIONAL LUNG CANCER AUDIT with manpower data for cardiothoracic surgery
Resection rates are higher in centres who treat more cases R = 0.155 p = 0.06
Resection rates are higher in base than in referring centres Across the UK Within each Cancer Network p < 0.001 p < 0.001 Resection Rate
Resection rates are higher in centres with 2 or more specialist thoracic surgeons p = 0.02 Resection Rate
Resection rates are higher when surgeons attend preoperative MDTs p = 0.012
The increase in resection rate was greatest in those units who employed new thoracic surgeons p = 0.04 19% 66% 2009 Growth Resection Rate 2008
Conclusion • Lung cancer resection rates in UK can be increased by • Increasing the number of specialist thoracic surgeons at preoperative MDTs in referring hospitals • Increasing the number of specialist thoracic surgeons in operating centres • Thereby increasing the individual caseload in any unit • Individual Units must invest in more pure Thoracic Surgical appointments • The number of specialist thoracic surgeons in training must be increased