Download

1 / 65
650 likes | 808 Views
HETV Partnership Council Thursday 3 July 9.30am – 2.30pm Milton Hill House Hotel Wifi network: ConferenceWiFi password: venues Fill in all fields DeVeres screen. Welcome Sandra Hatton Managing Director HETV. New Independent Chair and HETV Business Plan :.

E N D
HETV Partnership CouncilThursday 3 July9.30am – 2.30pmMilton Hill House HotelWifi network: ConferenceWiFipassword: venuesFill in all fields DeVeres screen
New Independent Chair and HETV Business Plan: • We welcome Professor John Caldwell as the new HETV Independent Chair • HETV Delivery Plan 2014/5 – sets out our priorities for delivery over 2014/15 in response deliver the HETV Workforce Strategy Tomorrow’s People, Today - circulated shortly
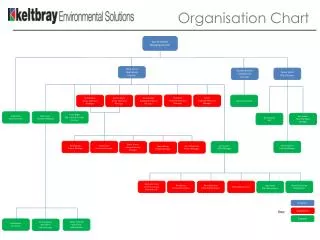
Strengthening HETV capacity: • Pauline Brown • Deputy Dir. Education & Quality • Quality • Performance • Juliet Anderson • Deputy Dir. Education • & Quality • Workforce strategy implementation • ECAT Plan • Programme Management Agnes Hibbert Programme Manager
Beyond Transition Realising our potential Health Education England
HEE Case for change: • We must create One HEE • Our operating model must allow HEE to focus on the whole workforce and transformation, increase efficient working and reduce duplication nationally • Increase governance expected of a Non-Departmental Public Body with greater alignment with the rest of the system • We must deliver the DoH requirements to reduce running costs by 20% (-£17m nationally) and the number of senior posts paid over £100k by at least the same amount • We must continue to be as efficient as possible in non-staff running costs to help meet our challenges
What does it mean for HETV? • Committed to maintaining the HETV Board and local delivery model, built on close stakeholder engagement and involvement • Opportunities for local providers to shape the workforce in support of patient needs • Better governance, better connections and efficiencies • New structures and management aligned across four regions, including new National Directors (Geography) • HETV Managing Director, Head of Finance and Director of Education & Quality roles cease to exist • Replaced by one Local Director role • Appointment of a Vice Chair to the HETV Board
Timetable • Engagement with staff/Boards now complete – final decisions made at HEE Board on 7 August • Statutory consultation of staff: • phase 1 (senior): July 2014 onwards • phase 2 (functions): October 2014 onwards • New senior team in place: 30 September 2014 • Complete and review: March 2015
Partnership Council review: • Final Partnership Council for 2014, ahead of Autumn Conference – Tuesday 14 October, The Oxford Hotel • This represents our sixth Partnership Council event – increasing audience, increasing representation and increasing influence on HETV
Partnership Council: You said, we listened, we did • November 2013: Our organisational effectiveness and Board composition. • We addressed your feedback – widening out Partnership Council to include more representation • We changed the composition of our Board – including local commissioners • We’ve increased regular communications to you and we want more feedback and involvement - @hethamesvalley on Twitter and our website
Partnership Council – February: You said, we listened, we did • February 2014: We discussed the refreshed HEE Mandate and how to meet it • We consulted on development of HETV Support Worker Strategy • Latest version approved by HETV Board in June • We responded to calls to ensure comprehensive approach to all roles • End-to-end approach across system • Develop a ‘Skills Partnership’ - get involved via Richard.Griffin@bucks.ac.uk
Partnership Council – May: You said, we listened, we did • May 2014: Discussed development of HETV’s Dementia Strategy and how we meet HEE Mandate target to roll-out Dementia Awareness Training • Your feedback has informed the training outcome framework • We responded to calls to build on existing work and to aid collaborations - Dementia Academic Action Group (DAAG) is now scoping all current provision of Dementia Training (reporting Sept 2014) • We will respond to calls for ‘blended approach’ in the second phase – development of new training materials for all staff • Our lead: zoe.scullard@thamesvalley.hee.nhs.uk and jacqueline.fairbairnplatt@thamesvalley.hee.nhs.uk
Partnership Council – July: Out of Hospital Care • Today, we discuss the need to move towards increased Care Closer to Home, with new out of hospital models • What are the impacts on our workforce? • How can HETV support you to ensure we have the right skills, right staff in the right place at the right time?
Workforce Planning County Consultation Groups • Share service commissioning plans – CCGs, Local Authorities • HETV will share latest workforce demand statistics and will report on 2015/16 education commissions - review and challenge • An opportunity to be involved in the development of the Education Commissioning & Training Plan 2015/16 • Buckinghamshire/Milton Keynes: 9.00am –1pm: Thursday 24 July Clare Foundation Centre • Oxfordshire: 9.00am – 1pm: Tuesday 29 July (note date/venue change) Marston Rd Campus, Oxford Brookes University • Berkshire: 9.00am – 1pm: Thursday 31 July Easthampstead Park, Bracknell
Purpose of Partnership Council and our ways of workingProfessor Peter HawkinsLead Facilitator
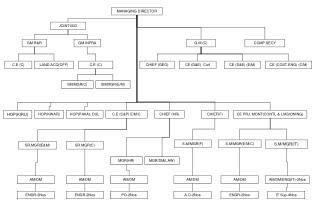
Government HEE Role of Partnership Council as an advisory body to HETV: HETV Board 2) The design process detailing the right route through which to gain the required information 3) The right cycle of timing to this process 1) Commissioning of high quality, well defined strategic questions Board members and their own organisations Local partnerships between HEIs/providers HETV Exec Partnership Council HETV Task & Finish Groups Expert stakeholder groups T&F specific stakeholder groups
The UK health challenge between now and 2032 • Population growth of 8 million • Half the population over 50 • Over 65s: 10.6 million – 16.1 million • Over 85s: 1.26 million – 2.6 million • Obesity: 26% - 40% • Arthritis: 8 million - 17 million • Dementia: 800,000 - 1.3 million • Dementia cost of care - £40 billion • Source Kings Fund: Renewal Associates
Objectives: • Hear from our keynote speakers perspectives on both the strategic drivers to a move towards Out of Hospital Care • Share good practice and hear from some of our local leaders in Out of Hospital Care delivery • Consider the workforce challenges and priorities • Discuss and inform how HETV and all local partners can work together to drive improvements
Keep the debate going: • Keep the debate going via the HETV Twitter feed @hethamesvalley – follow us • #hetvpartnershipcouncil
Out of Hospital Care - Responding to the Workforce ChallengesEmeritus Professor David Sines
Rationale: For staff across the health and social care system in the Thames Valley, the shift of care to the community will enable skills to be used more appropriately and deliver the highest quality care more effectively across organisational and professional boundaries. Particular focus is required on the skills, competencies and enhanced roles to be embedded in the community in order to successfully deliver the vision for out of hospital care.
Strategic workforce drivers: ‘We are moving away from a 20th century model with its outdated divisions of hospital-based practice and of ‘health’ and ‘social’ care… ‘....towards a 21st century system of integrated care, where clinicians work closely together in flexible teams, formed around the needs of patients and not driven by professional convenience or historic location’. RCGP – 2022 GP HEE 15-Year Strategic Framework
Rational and drivers: • HEE Mandate from Government – setting national priorities ‘The health and care system will require a greater emphasis on community, primary and multi-integrated health and care. Working in multi-disciplinary teams and work to break down barriers between primary and secondary care is required. HEE will train and develop a workforce with skills that are transferable between these different care settings.’ HEE Mandate
Rational and drivers: • Built around six Strategic Themes – including Care Closer to Home theme and Integrated Person-Centred Care • ‘90% of patient interactions take place in primary care, community settings and people’s own homes. We need to build skills and competencies in preventative care, to support • home-based care and to enable patients in self-care.’ HETV Workforce Strategy – Tomorrow’s People, Today
What could this mean for our workforce – both existing and for the future? Need more diverse multiprofessional roles underpinned by excellent clinical skills Even with greater productivity, primary care workforce needs to expand Patients and carers recognised as part of workforce and provided with support ....this will have to be supported by better collaboration between primary and community nursing GPs will continue to play the generalist role yet spend more time overseeing delivery of care by multi-disciplinary teams... Enhancing skills of the administrative staff to incorporate basic clinical tasks and more general advice and support for patients ... and some may also choose to augment additional clinical and leadership specialisations.
Developing the HETV Out of Hospital workstream – what is needed? • Understanding what innovative initiatives are there - identifying the workforce-specific considerations and sharing the good practice • Identifying the skills and competencies required to deliver these new services effectively • Identifying new roles, laying foundations for better succession planning and career development to attract, recruit and retain staff to the community setting • HETV to work closely local partners to ensure that education commissioning responds to local priorities to meet the shift • Building new partnerships – with social care, with Public Health, with private/voluntary/independent sectors • What else does HETV need to be doing to support and develop?
HETV next steps: • Today represents the launch by HETV of a new Out of Hospital Care Workforce workstream • 17 July – HETV Board will consider feedback and proposals developed from today’s meeting • A programme of activity will be developed within HETV, working closely with local and national partners • Take the opportunity today to help shape the development of this workstream
The strengths in the region: • The Thames Valley is well placed to deliver through: • A strong track record of integrated care initiatives across our designated localities and at every level of the system • Plans to shift care from acute to community settings, which will ensure financially sustainable delivery • The partnerships that have been established, working together to develop trust and consensus about what needs to change • Experience and understanding of the technical systemic changes that need to happen to make the difference to patients, service users and staff.
Making it happen: There are: “Those who make things happen; “Those who think they make things happen; “Those who watch things happen; “Those who wondered what happened; “Those who did not know anything had happened at all!”
Out of Hospital care clinical network – a critical area for success Dr Dan Lasserson MA MD FRCP Edin MRCGP Out of Hospital Care Clinical Network Lead, Oxford AHSN Senior Clinical Researcher, Nuffield Department of Primary Care Health Sciences, University of Oxford Senior Trust General Practitioner, Oxford University Hospitals NHS Trust
Focus of the Out of Hospital Care network • Acute illness in patients who live with frailty • Challenge of recognition and response • Timely • Assessment • Intervention • Monitoring • Patients at the centre of design of care
Development of alternative care pathways for acutely unwell adults • Emergency Multidisciplinary Unit (EMU) concept • Accessible, rapid, multidisciplinary diagnosis and treatment from a community setting • Medical – interface capability, drawn from 2°and 1°care clinicians • Nursing • Physiotherapy • Occupational therapy • Social work • Transport • Credible alternative to acute hospital admission
EMU operation • Catchment: 140k at 11 practices • Weekday working: 8am – 8pm • Weekend working: 10am – 4pm • Vertical integration: • Integration with ‘Hospital @ Home’ • Patient capture (111, 999) Referrals outside the hyperacute pathways – Chest Pain, Stroke, Fractured NOF
Investigations • Point of care bloods • Na, K, urea, creatinine, calcium, glucose, bicarbonate, gases, INR, haemoglobin, troponin, CRP • ECG • Plain X-Ray (no cross-sectional imaging) Interventions • ‘Interface MDT care’: delivers enabling care alongside interventions traditionally delivered in an acute hospital, in settings close to home • Intravenous fluid, antibiotics, diuresis, blood products Care pathways • Ambulatory care • Bed based care (community or acute)
Acutely unwell frail co-morbid adult living at home/care home Paramedic Primary Care Community team EMU referral
Acutely unwell frail co-morbid adult living at home/care home Paramedic Primary Care Community team EMU referral Dedicated transport EMU assessment and treatment
Acutely unwell frail co-morbid adult living at home/care home Paramedic Primary Care Community team EMU referral Dedicated transport EMU assessment and treatment Home Community hospital Acute hospital
Presentations • Breathlessness • Leg swelling • Global decline in function • Reduced mobility • Confusion • Collapse • Fall • Weight loss • Fever • Fatigue
Diagnoses Presentations • Breathlessness • Leg swelling • Global decline in function • Reduced mobility • Confusion • Collapse • Fall • Weight loss • Fever • Fatigue • Cardiac failure • PE • Respiratory tract infection • Cellulitis • Urinary tract infection • COPD exacerbation • Fast AF • Dehydration • Electrolyte disturbance • Pleural effusion • Acute kidney injury • Decompensated liver disease • Upper GI bleed • Medication side effects
Implementing the Silver Book • Respect for autonomy and dignity • Access to health and social care based on need • Integrated health and social care services delivered by interdisciplinary working • Rapid comprehensive geriatric assessment in response to frailty syndromes • Ambulatory emergency care pathways for those who do not require admission
Future care models at the interface of primary and secondary care
The axes of generalism Vertical generalism of traditional community practice
The axes of generalism Horizontal generalism -optimised care to an increasingly prevalent complex patient population
Network Partners • Care providers and commissioners • Academic partners – reflect breadth of acute care provision • Patients and the public • Third sector organisations
Out of Hospital care clinical network – a critical area for success Dr Dan Lasserson MA MD FRCP Edin MRCGP Out of Hospital Care Clinical Network Lead, Oxford AHSN Senior Clinical Researcher, Nuffield Department of Primary Care Health Sciences, University of Oxford Senior Trust General Practitioner, Oxford University Hospitals NHS Trust