Download
1 / 20
210 likes | 448 Views
differences. (a psychological conflict converted into a physical problem). SOMATIZATION DISORDERS. Hysterical. Preoccupation. conversion disorder. hypochondriasis. somatization disorder. BDD. pain disorder. suffer changes in physical functioning.

E N D
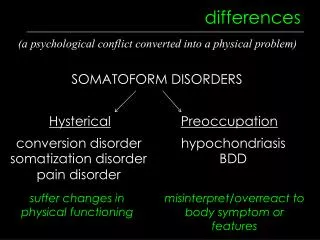
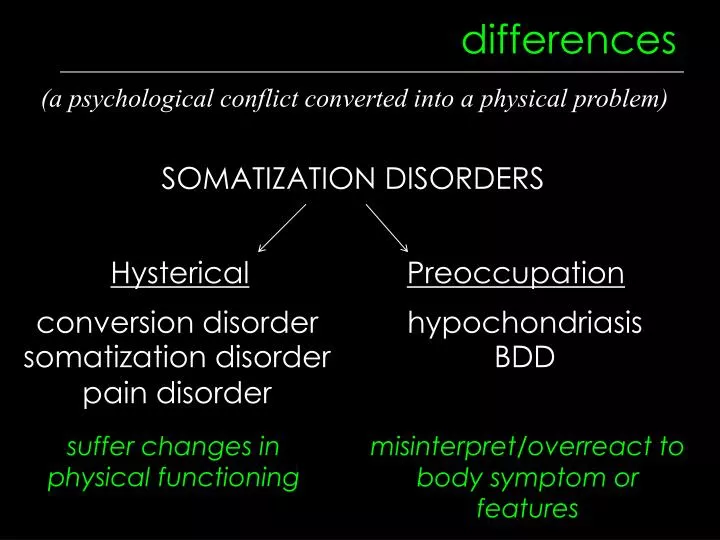
differences (a psychological conflict converted into a physical problem) SOMATIZATION DISORDERS Hysterical Preoccupation conversion disorder hypochondriasis somatization disorder BDD pain disorder suffer changes in physical functioning misinterpret/overreact to body symptom or features
purposely faking these are NOT somatization disorders Why do it? malingering factitious disorder to play the sick role; attn to gain profit or avoid work/jail time
conversion disorder DIAGNOSTIC CRITERIA • 1+ sensory or voluntary motor deficit • an associated stressor e.g. blindness, numbness, paralysis, gait, seizures, deafness, mutism STATS • .005% prevalence • onset: at time of extreme stress • sex ratio: 2-10:1 • course: resolves w/in 2 weeks after stressor
conversion disorder CAUSE a trauma where escape was needed but running away was not possible or acceptable (major mood disorder + severe stress event) • TREATMENT • therapy for original trauma • exposure to stimuli that “produce” symptoms • do not reinforce with attention • positive reinforcement when deficits go away • SSRIs
somatization disorder DIAGNOSTIC CRITERIA • before 30 yrs old, years of many long-lasting physical complaints (in excess or not explainable by GMC): • 4 pain • 2 gastro-intestinal • 1 sexual • 1 neurological/sensory/motor (just symptoms, not worried about a specific disease)
somatization disorder STATS • prevalence 4% • sex ratio: 2:1 • onset: adolescence • course: chronic • low SES, low edu, unmarried • runs in families (10-20% close female relatives are concordant)
somatization disorder CAUSE (genes for ASPD) impulsiveness – short term gain (attn) – long term probs (social isolation) pleasure-seeking – provocative sexual behavior TREATMENT teach how to interact & relate to others w/o relying on conversations about symptoms
pain disorder DIAGNOSTIC CRITERIA • pain in 1+ sites • not faked • associated w/ a stressor STATS • 5-12% prevalence • onset: any • can start from condition w/ real pain but persists TREATMENT • cognitive therapy & relaxation
hypochondriasis DIAGNOSTIC CRITERIA • 6+ months • preoccupied that has serious disease despite medical reassurance otherwise STATS • prevalence 1-5% • sex ratio: 1:1 • onset: early adulthood; trimodal (14,45,60+) • course: chronic but waxes & wanes
hypochondriasis CAUSE • modeling reinforcement by escaping circumstances, classical conditioning, cognitive misinterpretation of interoceptive sensation TREATMENT • SSRIs • cognitive therapy
body dysmorphic disorder DIAGNOSTIC CRITERIA • preoccupied w/ imagined defect or excessive concern over a defect STATS • 1-5% prevalence • sex ratio: 1:1 • onset: adolescence to 20’s • 30% are housebound, 17% attempt suicide • 50% comorbid w/ depression
body dysmorphic disorder TREATMENT • SSRIs • exposure & response prevention helps 80% • cognitive therapy ADDITIONAL DIAGNOSIS If firmly held, get “Delusional Disorder, Somatic Type”
purposely faking MALINGERING (external incentive) • avoid military duty • avoid incarceration • avoid work • gain insurance or lawsuit money
purposely faking FACTITIOUS DISORDER Wants attention & sympathy • associated features: • childhood exposure to extensive med treatment • childhood abuse or disruption • grudge against medical profession • worked in medical profession • dependent personality • no social supports
dissociative disorders (disruption in conscious awareness, perception, memory, or identity ) Dissociative Amnesia conscious awareness & memory Depersonalization Disorder DID conscious awareness, memory, & identity conscious awareness & perception
depersonalization disorder DIAGNOSTIC CRITERIA recurrent sense of detachment from thoughts or body (causes distress or impairment) MISC • depersonalization and/or derealization • mostly case study research • decreased emotional responsiveness • no treatments effective STATS • 1% prevalence • onset: 23 yrs average • course: chronic
dissociative amnesia DIAGNOSTIC CRITERIA 1+ episodes of memory loss (usually of trauma) (causes distress or impairment) “generalized” – no memory for ANYTHING including own identity “localized” – a.k.a. “selective”, can’t recall specific events or time period TREATMENT • remove from threatening situation, hypnosis, tranquilizers with therapy
dissociative fugue DIAGNOSTIC CRITERIA • sudden, unexpected travel from home/work w/ dissociative amnesia • confusion about identity (maybe new identity) TREATMENT • same
dissociative identity disorder DIAGNOSTIC CRITERIA • 2+ identities that recurrently take control • memory lapses MISC • identity, conscious awareness, & memory is fragmented • “alters”, “host”, & “switching” • alters are not full personalities • sex ratio: 3-9:1
dissociative identity disorder CAUSE • Post Traumatic Theory: • repeated traumatic abuse as child & autohypnotic dissociation as defense • develops by 9 yrs old (after PTSD likely) • Socio Cognitive Theory: • highly suggestible person learns to adopt & enact roles of identities due to clinician suggesting & reinforcing them TREATMENT reintegrate identities, hypnosis, show client videotape of alters