Download
1 / 19
240 likes | 689 Views
Vitamin K Sept 21. 2012. By: Anja Kovacevic Nina Krupetsky Larissa Boychuk Caitlin McIntyre . PHM142 Fall 2012 Instructor: Dr. Jeffrey Henderson. Types / Structure. Lipid- soluble Common 2-methyl-1,4-naphtoquinone ring Differ in structure at 3-position K1 plants

E N D
Vitamin KSept 21. 2012 By: Anja Kovacevic Nina Krupetsky Larissa Boychuk Caitlin McIntyre PHM142 Fall 2012 Instructor: Dr. Jeffrey Henderson
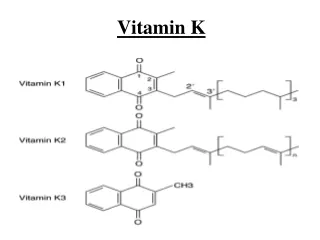
Types / Structure • Lipid- soluble • Common 2-methyl-1,4-naphtoquinone ring • Differ in structure at 3-position • K1plants • K2 bacteria in gastrointestinal tract
Function • Critical for: • Blood coagulation • Bone formation and remodelling • Recent evidence of its role in brain function, cell growth, apoptosis
Dietary Sources • Dietary Recommendation: 120 and 90µga day for adult males and females • K1: • Fruits and vegetables (especially leafy greens) • Spinach, cabbage, kale, cauliflower, broccoli, brussel sprouts, avocado, kiwi, grapes, parsley* • Certain Oils (soybean, canola, olive) • K2: • Meat • Eggs • Dairy http://www.home-remedies-and-natural-cures.com/vitamin-k.html
Deficiency • Rare in adults • Newborns – higher risk • Patients with liver damage or disease • Those with eating disorders • Those taking vitamin K antagonists (warfarin) • Signs/symptoms • Heavy menstrual bleeding, anemia, nose bleeds, osteoperosis, coronary heart disease • In infants - intracranial hemorrhage
Vitamin K is essential for biochemical synthesis of factors: • IX • VII • X Essential for converstion of Prothrombin to Thrombin • Prothrombin and the other cofactors are serine proteases http://blogs.scientificamerican.com/the-curious-wavefunction/2012/07/27/gene-duplication-frees-up-enzymes-for-molecular-promiscuity/
Why is Vitamin K important? • synthesized in the liver and then secreted into the circulation as inactive forms (zymogens) • Vitamin K-dependent carboxylation of glutamic acid (Glu) residues forms γ-carboxyglutamic acid (Gla) • Gla residues aid in the chelation of calcium ions and ensure these clotting proteins can bind to platelets and endothelial cells.
What does Vitamin K do? • Carboxylated Prothrombin can bind Ca2+; which is essential for its activation to Thrombin. • Abnormal Prothrombin cannot bind Ca2+; prohibiting the clotting cascade.
Biosynthesis of GluGla (2) Glu (1) (3) Gla (4)
Biosynthesis of Glu Gla (3) CO2 is added to the γ-carbon of glutamic acid to form γ-carboxyglutamic acid ENZYME: Vitamin K-dependent Carboxylase
Biosynthesis of GluGla (2) Glu (1) (3) Gla (4)
Why does the body recycle Vitamin K? • Very minimal body stores • Must have regular dietary intake • Recycles so that the same vitamin K can be cycled and re-used many times (decreasing need in dietary intake)
Warfarin and Vitamin K • Warfarin blocks vitamin K recycling and activation (by inhibiting 2 reductase) therefore, carboxylation of glutamic acid cannot occur at a normal rate • This decreases blood coagulation. anticoagulant. • Warfarin is a Vitamin K antagonist.
Warfarin Blocks 2 Pathways • (1) Blocks Quinone Reductase • Vitamin K’s activation to Vitamin K hydroquinone (2) Blocks Vitamin K-epoxide reductase Vitamin K (epoxide) recycling to Vitamin K
Role of Vitamin K in Bone Formation • Vitamin K is a cofactor for the γ-carboxylation of osteocalcin, a protein found in bone tissue • Osteocalcin is involved in the mineralization of bone matrix • γ-carboxylation of Glu residues to Gla gives each osteocalcin molecule the ability to bind Ca2+ and form part of the mineralizing bone matrix • Non-carboxylated osteocalcin cannot form bone • Serum osteocalcin is used as a biochemical marker of bone formation
Vitamin K and Osteoporosis • Inadequate Vitamin K intake has been linked to osteoporosis and an increased incidence of hip fracture in the elderly • Under-carboxylated osteocalcin in blood serum is an indicator of Vitamin K deficiency and may indicate a higher risk of fracture • Studies of the benefits of Vitamin K supplementation in osteoporosis have been inconclusive • Further research into exact biochemical mechanisms is necessary
SUMMARY SLIDE • The two naturally-occurring types of Vitamin K are K1 & K2, synthesized by plants and gastrointestinal bacteria, respectively. • Vitamin K deficiency is rare in healthy adults but is dangerous in infants where it can cause hemorrhaging in vital organs such as the brain • Vitamin K is essential for the synthesis of factors VII, IX, X and for the conversion of prothrombin to thrombin • The γ-carboxyglutamic acid on prothrombin can bind Ca2+ allowing for the conversion to thrombin • Vitamin K Hydroquinone (active form), is a cofactor of the enzyme γ -glutamyl carboxylase; leads to carboxylation of Glu to Gla • The vitamin K is recycled • Warfarin is a vitamin K antagonist in btoh bone mineralization and coagulation • Blocks the acitvation and recycling of vitamin K • Vitamin K is needed for γ-carboxylation of Glu→Gla residues on osteocalcin; Gla binding Ca2+ helps osteocalcin incorporate into mineralizing bone • Vitamin K deficiency has been linked to osteoporosis for a long time, but the evidence is not definitive since exact biochemical mechanisms are not yet known
References • Booth SL, Dallal G, Shea MK, Gundberg C, Peterson JW, Dawson-Hughes B. (2008) Effect of vitamin K supplementation on bone loss in elderly men and women. J Clin Endocrinol Metab. 93(4):1217-1223. • Booth SL, Suttie JW. (1998) Dietary intake and adequacy of vitamin K. J Nutr. 128(5):785-788. • Booth SL, Tucker KL, Chen H, et al. (2000) Dietary vitamin K intakes are associated with hip fracture but not with bone mineral density in elderly men and women. Am J Clin Nutr. 71(5):1201-1208. • Ferland G. (2012) Vitamin K, an emerging nutrient in brain function. Biofactors. 38(2):151-157 • Furie B, Bouchard BA, Furie BC. Vitamin K-dependent biosynthesis of gamma-carboxyglutamic acid. Blood. 1999;93(6):1798-1808 • Xing Gong, Ramana Gutala, Anil K. Jaiswa, Quinone Oxidoreductases and Vitamin K Metabolis, Vitamins & Hormones, Volume 78, 2008, Pages 85–101 • Robins SP. 2012 “Biochemical Markers for Assessing Skeletal Growth” http://archive.unu.edu/unupress/food2/UID06E/UID06E1B.HTM • Saxena SP, Israels ED, Israels LG. (2001) Novel Vitamin K-dependent pathways regulating cell survival. Apoptosis. 6: 57-68. • Shearer MJ. (1997) The roles of vitamins D and K in bone health and osteoporosis prevention. Proc Nutr Soc. 56(3):915-937. • Vergnaud P, Garnero P, Meunier PJ, Breart G, Kamihagi K, Delmas PD. (1997) Undercarboxylated osteocalcin measured with a specific immunoassay predicts hip fracture in elderly women: the EPIDOS Study. J Clin Endocrinol Metab. 82(3):719-724. • Weber P. (2001) Vitamin K and Bone Health. Nutrition 17(10):880-887.