Download
1 / 58
690 likes | 1.57k Views
Fat Soluble Vitamins Vitamin A Vitamin E Vitamin D Vitamin K. Vitamin A. RETINOIDS. The retinoids : a family of molecules that are related to retinol (vitamin A) ------------------------------------- The term retinoids includes

E N D
Fat Soluble Vitamins Vitamin A Vitamin E Vitamin D Vitamin K
RETINOIDS The retinoids: a family of molecules that are related to retinol (vitamin A) ------------------------------------- The term retinoids includes natural & synthetic forms of vitamin Athat may or may not show vitamin A activity
Retinoids 1- Retinol A primary alchol containing b-ionone ring with an unsaturated side chain. It is found in animaltissues as a retinyl ester with long-chain fatty acids. 2- Retinal The aldhyde derived from the oxidation of retinol. Retinol and retinal canbeinterconverted.
3-Retinoic acid The acid derived from oxidation of retinal. It can not be reduced in the body, and therefore, can not give rise to either retinal or retinol 4-b-carotene Plantfoods contain b-carotene, which can be oxidatively cleaved in the intestine to yield two moleculesofretinal In humans, the conversion is insufficient, and vitamin A activity of b-carotene is only about one sixth of that of retinol
Absorption & Transport of vitamin A Transport to the Liver I- Retinol is derived from (DIET SOURCES) 1-DIET Retinyl esters (animal source) which are hydrolyzed in the intestinal mucosa, releasing retinol and free fatty acids 2- DIET b-carotenes(plant source) which is cleaved 2 retinal retinol II- Retinol is esterified with fatty acids to give retinyl esters III-Retinyl esters are collected by the chylomicrons into the lymphatic system. IV- Retinyl esters contained in the chylomicrons are taken up and stored by the liver
Release from the Liver • When needed, retinol is released from the liver and transported to extra hepatic tissue by plasmaretinol binding protein(RBP) • Theretinol - RBP complex attaches to specific receptors on the surface of the cells of peripheral tissues permitting retinol to enter
Mechanism of Action of vitamin A • Retinol is oxidized to retinoic acid inside cells. • Retinoic acid binds with high-affinity to specific receptor proteins present in the nucleus of target tissue, such as epithelial cell. • The activated retinoic acid - receptor complex interacts with nuclear chromatin (genes) to stimulate retinoid-specific mRNA synthesis, resulting in the production of specific proteins that mediate several physiological functions. e.g. retinoids control the expression of keratin gene in most epithelial tissues.
Functions of Vitamin A • Vision • Growth • Reproduction • Epithelial cells maintenance
Functions of Vitamin A 1-Vision • Vitamin A is a component of the visual pigments of rodand cone cells. • Rhodopsin, the visual pigment of the rod cells in the retina, (for vision in dim light) consists of 11-cis retinal specially bound to the protein opsin. • When rhodopsin is exposed to light, a series of photochemical isomerization occurs, which results in release of all trans retinal and opsin (with bleaching of the visual pigment). • This process triggers a nerve impulse that is transmitted by the optic nerve to the brain. • Regeneration of rhodopsin requires isomerization of all trans retinal back to 11-cis retinal, which spontaneously combines with opsin to form rhodopsin.
2- Growth • Vitamin A is essential for normal growth of cells (by synthesis of important proteins) • bone growth is slow in vitamin A deficiency. • Animals deprived of vitamin A suffers keratinzation of taste buds leading to losing of their appetites.
3-Reproduction • Retinol & retinalare essential for normal reproduction 1- supporting spermatogenesis in males 2- preventing fetal resorption in females • Retinoic acid is inactive in maintaining reproduction & the visual cycle, BUT promotes growth. Thus, retinoic acids given only since birth to animals, leads to blindness & sterility. 4-Epithelial cells maintenance • Vitamin A is essential for normal differentiation of epithelial tissues and mucus secretion.
Distribution of Vitamin A • Sources of retinol(retinyl esters) : animal source Liver, kidney, cream, butter & egg yolk • Sources of carotenes(precursors of vitamin A) : plant source Yellow & dark green vegetables & fruits Requirement for Vitamin A • One RE (retinol equivalents) = 1mg of retinol 6mg of b-carotene 12mg of other carotenoids • RDA for adults 1000 RE for males 800RE for females
Clinical indications 1-Dietary deficiency Vitamin A, administered asretinolor retinyl esters, is used to treat patients deficient in the vitamin (not retinoic acid) Night blindness One of the earliest signs of vitamin A deficiency Difficulty in seeing in dim light. Prolonged deficiency leads to irreversible loss of visual cell. (affection of rods of retina) Xerophthalmia Severe deficiency of vitamin A Pathological dryness of the epithelium conjunctiva & cornea. It may end in corneal ulcerations and blindness.
2-Acne & Psoriasis Dermatologic problems of acne and psoriasis are effectively treated with retinoic acid or its derivatives. • Mild cases of acne is treated by topical application of tretinoin (All trans retinoic acid) which is too toxic for systemic administration. • Severe recalcitrant cystic acne unresponsive to conventional therapies, isotretinoin(13-cis retinoic acid) is administered orally
3-Prevention of chronic diseases • Populations consuming diets high in b-carotene show decreased incidence of heart diseases & lung & skin cancer • Consumption of foods rich in b-carotene is associated with reduced risk of cataracts and macular degeneration
Toxicity of Retinoids I. Vitamin A excess(hypervitaminosis A syndrome) Amounts exceeding 7.5 mg/day of retinol 1- Excessive intake of vitamin A may cause the followings: • dry skin & pruiritis are early signs • liver enlarged, cirrhotic • increased intracranial pressure (mimic symptoms of brain tumours e.g. headache etc…) 2-Pregnant females should not ingest excessive amounts of vitamin A because of its potential for causing congenital malformations in developing fetus.
II. Isotretinoin drug(13-cis retinoic acid) 1-Teratogenic • So, absolutely contraindicated in women with childbearing potential. • Pregnancy should be excluded before initiation of treatment & adequate contraceptive (birth control) must be used 2-Risk of coronary heart diseases Prolonged treatment with 13-cis retinoic acid leads to hyperlipidemia & increase in LDL/HDL ratio with increased risk of coronary heart diseases.
Vitamin E • E vitamins consist of 8 naturally occurring tocopherols, of which - tocopherol is the most active. • The primary function of vitamin E is an antioxidantin prevention of the nonenzymic oxidation of cell components as polyunsaturated fatty acids by molecular O2 & free radicals.
Distribution & requirements of vitamin E • Vegetable oils are rich sources (plant sources) • Liver& eggs contain moderate amounts (animal sources) • RDA for a-tocopherol is 10 mg for men 8 mg for women • Requirement is increased with increased intake of polyunsaturated fatty acids.
Deficiency of vitamin E • Deficiency of vitamin E is almost entirely restricted to premature infants. • In adults, it is usually associated with defective lipid absorption or transport. • Signs of vitamin E deficiency include sensitivity of RBCs to peroxide & appearance of abnormal cellular membrane.
Clinical indications Vitamin E is notrecommended for the prevention of chronic disease, such as coronary heart disease or cancer. Subjects in the Alpha-Tocopherol, Beta Carotene Cancer Prevention Study trial who received high doses of vitamin E, not only lack cardiovascular benefit but also had an increased incidence of stroke. Toxicity of vitamin E:no toxicity at 300mg / day dose
Vitamin D • The D vitamins are a group of sterols that have a hormone-like function. • The active molecule, 1,25-dihydroxycholecalciferol (1,25-di OH D3 ), binds to intracellular receptor protein. • The 1,25-diOH D3 - receptor complex interacts with DNA in the nucleus of target cells, and either stimulates gene expression, or represses gene transcription. • The main actions of 1,25-diOH D3 are to regulate plasma levels of calcium & phosphorous.
Distribution of vitamin D: (Sources) 1- Diet • Ergocalceferol (vitamin D2) is found in plants • Cholecalceferol (vitamin D3) is found in animaltissues. 2- Endogenous vitamin precursors 7-Dehydrocholesterol, is converted tocholecalceferol (vitamin D3) in the dermis and epidermis of human skin exposed to sunlight. Individuals with limited exposure to sunlight require performed vitamin D
Metabolism of vitamin D 1- Formation of 1, 25 dihydroxycholecalceferol (1,25-diOH D3) • Vitamin D2 & D3 are not biologically active • but are converted in vivo to the active form of D vitamin by two sequential hydroxylation reactions (two hydroxylases) that require monooxygenase, molecular oxygen and NADPH. The two hydroxylases uses cytochrome P450
First Hydroxylation • occurs at the position 25 • catalyzed by a specific hydroxylase in the liver • to give 25 hydroxycholecalceferol (25-OH D3) - the predominant form of vitamin D in plasma - the major storage form of the vitamin
Second Hydroxylation • 25-OH D3 is further hydroxylated at position 1 • by the enzyme specific 25-hydroxycholecalceferol 1-hydroxylase • found primarily in the kidney • resulting in the formation of 1, 25 dihydroxycholecalceferol(1,25 diOH D3) is the most active vitamin D metabolite
2-Regulation of 1-hydroxylase • Its formation is regulated by the level of plasma calcium and phosphate levels in plasma. • 1-hydroxylase activity is increased: • DIRECTLY by low phosphate • INDIRECTELY by low calcium levels (hypocalcemia) release of Parathyroid Hormone (PTH) activation of 1 hydroxylase increased production of 1,25-di(OH) D3
Function of Vitamin D The overall function of 1,25-diOH D3 is to maintain adequate plasma levels of calcium. It performs this function by • increasing uptake of calcium by the intestine • minimizing loss of calcium by the kidney • stimulating resorption of bone (when necessary)
1-Effect of vitamin D on INTESTINE: • 1, 25-diOH D3stimulates intestinal absorption of calcium & phosphate. • 1,25-diOH D3 enters intestinal cell and binds to cytosolic receptor 1,25-diOH D3 – receptor complex to nucleus selectively interacts with DNA increased synthesis of specific calcium-binding protein enhanced Calcium Uptake
2-Effect of vitamin D on BONE: 1,25-diOH D3 stimulates the mobilization of calcium and phosphate from bone by a process that requires PTH increase inplasma calcium & phosphate
Distribution & Requirement of vitamin D • Vitamin D(Cholecalcerferol) occurs naturally in fatty fish, liver, and egg yolk. • Milk is not a good source for vitamin D (unless if fortified). • The RDA for adults is 200 IUvitamin D [available in 5 mgcholecalceferol (vitamin D3)]
Clinical indications 1- Nutritional Rickets Vitamin D deficiency net demineralizationof bone Rickets(in children)Osteomalacia(in adults)
Rickets thecontinued formation of the collagen matrix BUT incomplete mineralization softbones deformity Osteomalacia demineralization of preexisting bones susceptibility tofracture
Causes of vitamin D deficiency (one or bothof the following causes) 1- Insufficient exposure to daylight(sunlight). 2- Deficiencies in vitamin D consumption In areas where sunlight is not sufficient RDA should be increased up to 800 IU/day instead of 200 IU/day (5 mg cholecalceferol) to reduce the incidence of osteoprotic fractures
2- Renal Rickets(renal osteodystrophy) The disorder results from chronic renal failure (with activity of 1-hydroxylase) decreased ability to form the active form of the vitamin (1,25-diOH D3) Treatment: 1,25-diOH D3 (calcitriol)
3- Hypoparathyroidism ( PTH) Deficiency or absence of parathyroid hormone (PTH) causes hypocalcemia and hyperphosphatemia. Treatment: any form ofvitamin D+ PTH
Toxicity of vitamin D • Vitamin D is the most toxic of all vitamins. • Vitamin D can be stored in the body and is only slowly metabolized • High doses (100,000 IU for weeks or months) can cause: loss of appetite, nausea, thirst and stupor • Enhanced calcium absorption and bone resorption results in hypercalcemia, which can lead to deposition of calcium in many organs, particularly the arteries and kidneys
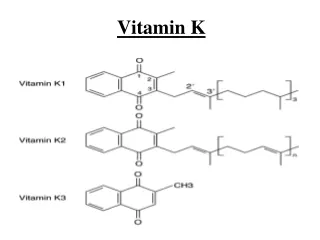
Vitamin K Some forms of vitamin K: 1- in plants as phylloquinone (vitamin K1) 2- in intestinal bacterial floras as menaquinone (vitaminK2) 3-syntheticderivative of vitamin K (menadione )
Function of vitamin K 1-Formation of gamma carboxyglutamate • Vitamin K is required in the hepatic synthesis of prothrombin and blood clotting factors II, VII, IXand X. • These proteins are synthesized as inactive precursor molecules. • Formation of clotting factors requires the vitamin K-dependentcarboxylation of glutamic acid residues • This forms a mature clotting factor that contains g carboxyglutamate (Gla), which are active clotting factors.
The action of vitamin K can beinhibitedby the following anticoagulants: • Dicumarol: natural, available in some plants • Warfaryn:a synthetic analog of vitamin K