Download
1 / 26
280 likes | 461 Views
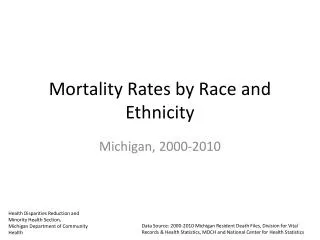
B reedtestrategie. CCR2 V64I polymorphism: morbidity and mortality in PREVEND. 18-04-2005 Mike Zuurman, Department of Internal Medicine, Section Nephrology University Medical Centre Groningen, The Netherlands. Chemokines and their receptors: families.

E N D
Breedtestrategie CCR2 V64I polymorphism: morbidity and mortality in PREVEND 18-04-2005 Mike Zuurman, Department of Internal Medicine, Section NephrologyUniversity Medical Centre Groningen, The Netherlands
Chemokines and their receptors: families Classified based on position of conserved cystein residues in the protein structure
CC-motif chemokine receptors: nomenclature Human Mouse Rat Historical names CCR1 Ccr1 Ccr1 CMKBR1, CC-CKR1, HM145, MIP-1a-R, RANTES-R, LD78-R - Ccr1l1 - CMKBR1L1, CC-CKR1-like 1, MIP-1a-R-like 1 CCR2 Ccr2 Ccr2 CMKBR2, CC-CKR2, CCR2A, CCR2B, MCP-1-R, mJE-R CCR3 Ccr3 Cmkbr3 CMKBR3, CC-CKR3, CC-CKR1-like 2, MIP-1a-R-like 2, eotaxin receptor CCR4 Ccr4 Ccr4 CMKBR4, CC-CKR-4, K5-5 CCR5 Ccr5 Ccr5 CMKBR5, CC-CKR5, ChemR13, CD195, HIV-1 fusion coreceptor CCR6 Ccr6 Ccr6 CMKBR6, STRL22, GPR29, GPR-CY4, CKR-L3, DRY6, LARC-R CCR7 Ccr7 Ccr7 CMKBR7, BLR2, EBI1, CDw197, AMG1 CCR8 Ccr8 - CMKBR8, CMKBRL2, CKR-L1, TER1, GPR-CY6, ChemR1, CC CKR-type 2 CCR9 Ccr9 Ccr9 CMKBR9, GPR-9-6, CC-CKR-9, CCR9A, CCR9B< GPR2 Gpr2 - CCR10, CCR9, CCR10A, CCR10B CCRL1 Ccrl1 - CCR11, VSHK1, CCBP2, CCX-CKR, GPCR14 CCRL1P - - - CCRL2 Ccrl2 - CC CKR-like 2, HCR, CRAM-A, CRAM-B, CKRX, E01, L-CCR HRH4 Hrh4 Hrh4 histamine receptor H4, HH4R, GPRv53, GPCR105 FPRL1 Fprl1 Fprl1 formyl peptide receptor-like 1, HM63, lipoxin A4-R, FPR2A, FMLP-R-II, Lxa4r
Chemokines Chemokine function: classical Chemokines
Chemokine function: recent • Intercellular communication (brain) • Angiogenesis (f.i. tumour related) • Orchestration of the immune response • * Pro- and anti-inflammatory • -Hematopoiesis • -Organogenesis • -Ovulation, luteal regression
Chemokines in pathology: renal disease J Am Soc Nephrol 11: 152-176, 2000
CC-motif chemokine receptor 2 comes in two flavours Ligands: -MCP-1 (CCL2) -MCP-2 -MCP-3 -MCP-4 -MCP-5 Nakayama et al.,AIDS 2004 Mar 26;18(5):729-38.
CCR2 64I: a single nucleotide polymorphism (SNP) Gives rise to a valine to isoleucine substitution
Literature on CCR2 64I and clinical outcome CCR2 64I is associated with reduced coronary artery calcification suggesting increased risk of unstable plaques (Valdes et al., ATVB 22, 2002) CCR2 64I is associated with higher prevalence of myocardial infarction (Ortlebb et al., J Mol Med 81, 2003; Petrkova et al., Immunol. Letters, 88, 2003) The minor allele (I) is associated with delayed progression to AIDS in HIV-1patients (Smith et al., Science 277, 1997) CCR2 64I shows no protective effect on death after development of AIDS in adults (Ioannidis et al., Ann Intern Med 135, 2001) CCR2 64I is associated with increased mortality in HIV-1 infected neonates after a survival period of 6 years (Ioannidis et al., J Med Genet. 41, 2004) Risk of acute renal transplant rejection was reduced in carriers of the CCR2-64I allele (Abdi et al., JASN 13, 2002)
CCR2 64I and receptor function • Initially scientists saw no apparent function difference between CCR2 64Vand CCR2 64I (chemotaxis, intracellular Ca2+ , ligand-binding etc.) • However, classically scientists examined CCR2B, and not CCR2A due to historical results that suggested much lower expression of CCR2A in monocytes Increasing evidence shows CCR2A and CCR2B expression depends on microenvironment ! For instance: * CCR2A ++ in myopathy (Bartoli et al., Acta Neuropath. 102, 2001) * CCR2B ++ in monocytic cellines (Tanaka et al., BBRC 290, 2002) • Indeed, Nakayama et al.(2004) showed neatly that the CCR2A and NOT CCR2B functionality is influenced by the valine to isoleucine substitution: - Increased surface expression of CCR2A - More stable expression of CCR2A - Increased down-regulation of CCR5, the principle co-receptor required by HIV-1 for infection
Previous studies only in patient populations already predisposed with CV-disease CCR2 64I and general population? What about predisposed cardiovascular morbidity? What about mortality?
Prevention of REnal and Vascular ENd-organ Damage Populatie Groningen 85000 individuals 40000 urine samples 8500 in preclinic (MA enriched) Genotyping Phenotyping
Baseline differences between hypertensives and normotensives in the study population BMI, body-mass index; MAP, mean arterial pressure; LLD, lipid lowering drugs; UAE: urinary albumin excretion. Continuous values show mean and standard deviation, except for UAE (median and 25th – 75th percentile). a: ANOVA P-value < 0.05; b: Pearson Chi square P-value < 0.05; c: Mann-Whitney U-test P-value < 0.05.
Characteristics of hyper- and normotensives by CCR2-V64I
* 30 VV II+IV 20 % 10 0 Non-hypertensives Hypertensives Prevalence of cardiovascular events during follow-up 12 VI + II VV 10 8 % of genotype group 6 4 2 0 1 2 3 4 5 Number of CE
Relative risk of cardiovascular events in hyper- and normotensive CCR2V64I I-carriers versus VV homozygotes. RR: relative risk, P: P-value of the genotype term in the logistic regression analyes. The full model includes, besides subject age, significant contribution of: usage of lipid-lowering drugs, sex, HDL-cholesterol, LDL+VLDL-cholesterol, mean arterial pressure and urinary albumin excretion..
Conclusion: CCR2 64I associates with CV-events when subjects already suffer from hypertension
Baseline characteristics and risk factors for mortality according to CCR2-V64I genotype
Table 2. Distribution of Causes of Death (COD) among CCR2-V64I genotype, subdivided in Malignant COD, Cardiovascular COD and Other (unrelated) COD.
All-cause mortality hazard ratios of CCR2 VI subjects using Cox regression models and CCR2V64I VV-individuals as reference.
Conclusions: 1. CCR2 64I associates with CV-events when subjects already suffer from hypertension 2. CCR2 64I associates with all-cause mortality, but does not predict CV-mortality 3. Results suggest an association of CCR2 64I with cancer-related mortality
Acknowledgements Medical Biology Gerrit van der Steege Elvira Oosterom Marcel Mulder Ron Korstanje Trial Coordination Centre Hans HillegeInternal Medicine, Nephrology Gerjan Navis Paul E. De Jong