Download
1 / 2

E N D
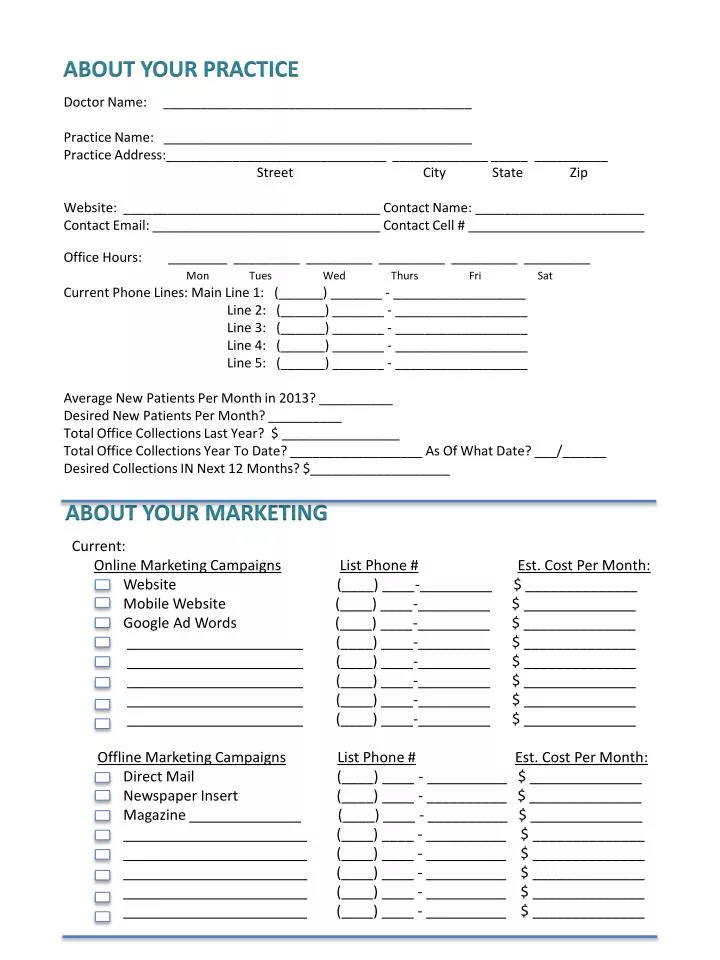
ABOUT YOUR PRACTICE Doctor Name: __________________________________________Practice Name: __________________________________________Practice Address:______________________________ _____________ _____ __________ Street City State ZipWebsite: ___________________________________ Contact Name: _______________________Contact Email: _______________________________ Contact Cell # ________________________Office Hours: ________ _________ _________ _________ _________ _________ Mon Tues Wed Thurs Fri SatCurrent Phone Lines: Main Line 1: (______) _______ - __________________ Line 2: (______) _______ - __________________ Line 3: (______) _______ - __________________ Line 4: (______) _______ - __________________ Line 5: (______) _______ - __________________Average New Patients Per Month in 2013? __________Desired New Patients Per Month? __________Total Office Collections Last Year? $ ________________Total Office Collections Year To Date? __________________ As Of What Date? ___/______Desired Collections IN Next 12 Months? $___________________ ABOUT YOUR MARKETING Current: Online Marketing CampaignsList Phone #Est. Cost Per Month: Website (____) ____-_________ $ ______________ Mobile Website (____) ____-_________ $ ______________ Google Ad Words (____) ____-_________ $ ______________ ______________________ (____) ____-_________ $ ______________ ______________________ (____) ____-_________ $ ______________ ______________________ (____) ____-_________ $ ______________ ______________________ (____) ____-_________ $ ______________ ______________________ (____) ____-_________ $ ______________ Offline Marketing CampaignsList Phone #Est. Cost Per Month: Direct Mail (____) ____ - __________ $ ______________ Newspaper Insert (____) ____ - __________ $ ______________ Magazine ______________ (____) ____ - __________ $ ______________ _______________________ (____) ____ - __________ $ ______________ _______________________ (____) ____ - __________ $ ______________ _______________________ (____) ____ - __________ $ ______________ _______________________ (____) ____ - __________ $ ______________ _______________________ (____) ____ - __________ $ ______________
MISSED CALL FEATURE – Text sent to mobile device Cell Phone To Send Text Message To: (_______) ________ - __________________ Do you what to be alerted 24/7 Yes No If No, please specify hours to be alerted: Monday From ________ until ________ Tuesday From ________ until ________ Wednesday From ________ until ________ Thursday From ________ until ________ Friday From ________ until ________ Saturday From ________ until ________ Sunday From ________ until ________ PAYMENT INFORMATION Type: Visa MC AMEX __________________________ Card #: ___________________________________ Exp Date ____ / _____ CVV _____ Name On Card: __________________________________________ Billing Address: ______________________________ ______________ ___ __________ Street City State Zip