Download
1 / 39
400 likes | 464 Views
T heme of lecture : ACQUIRED INTESTINAL ILEUS. ACQUIRED INTESTINAL ILEUS Classification. Causes of paralytic ileus. Abdominal trauma Abdominal surgery (i.e. laparatomy ) Serum electrolyte abnormality 1. Hypokalemia 2. Hyponatremia 3. Hypomagnesemia

E N D
Causes of paralytic ileus • Abdominal trauma • Abdominal surgery (i.e. laparatomy) • Serum electrolyte abnormality 1. Hypokalemia 2. Hyponatremia 3. Hypomagnesemia 4. Hypermagensemia D. Infectious, Inflammatory or irritation (bile, blood) 1. Intrathoracic • Pneumonia • Lower lobe rib fractures • Myocardial Infarction 2. Intrapelvic (Pelvic Inflammatory Disease) 3. Intraabdominal • Appendicitis • Diverticulitis • Nephrolithiasis • Cholecystitis • Pancreatitis • Perforated Duodenal Ulcer E. Intestinal Ischemia • Mesenteric embolism, ischemia or thrombosis F. Skeletal injury • Rib fracture • Vertebral fracture (e.g. lumbar compression fracture) G. Medications • Narcotics • Phenothiazines • Diltiazem or Verapamil • Clozapine • Anticholinergic Medications
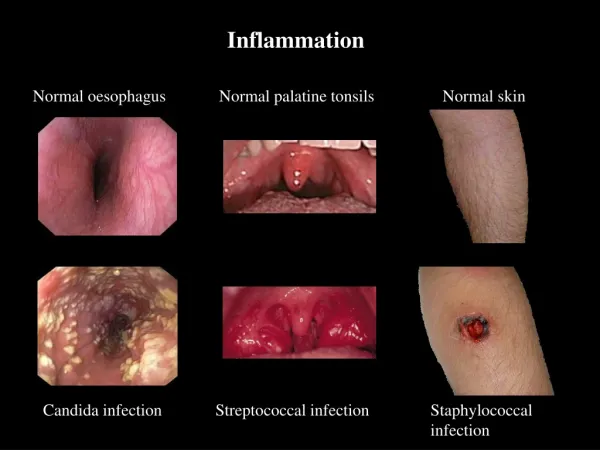
Clinical manifestations and diagnostic studies • Constant gnawing pain • repeated vomiting • symmetric abdominal distention • reduced or absence of peristalsis • increasing meteriorism • constipation • heavy intoxication
Treatment of paralytic ileus • Para-nephral and pre-sacral novocaine nerve blocks • Gastric lavage and intestinal intubation • Stimulation of intestinal peristalsis • IV fluids and electrolytes, • a minimal amount of sedatives, • adequate serum K level (> 4 mEq/L [> 4 mmol/L]) • Sometimes colonic ileus can be relieved by colonoscopic decompression; rarely cecostomy is required. Ileus persisting > 1 wk probably has a mechanical obstructive cause, and laparotomy should be considered.
Paralytic ileus Plain film in a case with Small bowel obstruction Post op Paralytic Ileus • Multiple dilated small bowel loops are seen (white arrowheads). • There is fecal material in the right and left colon(arrows). • Air is seen in the rectum. • The surgical staples indicate recent abdominal surgery. (black arrowheads).
Radiological findings of small bowel obstruction The characteristics of small bowel obstruction include: • Multiple air-fluid levels • Stacked • Centrally located loops of intestine • Dilated small bowel greater than 3 cms visible with valvulaeconniventes. • String of pearl sign caused by slow resorption of intraluminal air leaving small air bubbles trapped between valvulaeconniventes • Absence or paucity of colon gas: Collapsed colon
Radiological findings of large bowel obstruction The characteristics of small bowel obstruction include: • Obstructed colon usually appears as a peripherally located distended bowel with haustral markings. • No air distal to site of obstruction. • Sometimes the mass may be seen.
Adhesive Intestinal Obstruction The incidence of postoperative adhesive obstruction after laparotomy is about 2%. The procedures which have highest risk for adhesive McBurney’s point in pediatric patients are: • 1. subtotal colectomy, • 2. resection of symptomatic Meckel’s diverticulum, • 3. Ladd’s procedure, and • 4. nephrectomy.
Clinical Presentation • cramping abdominal pain, • distension, and vomiting.(bilious or even feculent). • Inspection of the abdomen may reveal obvious dilated loops of bowel and distension. • fever, tachycardia, decreased blood pressure, abdominal tenderness and leukocytosis.
Differential diagnosis • pancreatitis, • hepatitis • biliary tract disease. • urinary tract infection, nephritis, stones. • systemic infection. • colitis, rotavirus. • pneumonia.
Treatment • isotonic saline solutions, • nasogastric decompression, • correction of electrolyte abnormalities, • IV antibiotics, Indications for operation include obstipationfor 24 hours, continued abdominal pain with fever and tachycardia, decreased bloodpressure, increasing abdominal tenderness, and leukocytosis despite adequate resuscitationand medical treatment.The abdomen is opened through a previous incision, if present, and midline, ifnot. The cecum is identified and the collapsed ileum is followed proximally untildilated bowel and the point of obstruction is identified. The offending adhesivebands are disrupted and the abdomen is closed. Laparoscopic lysis of adhesions isanother option and may allow a shorter postoperative recovery and hospital stay.Postoperatively, nasogastric decompression and intravenous fluids are continueduntil return of bowel function and the volume of gastric aspirate decreases.
Supine view of the abdomen in a patient with intestinal obstruction. Dilated loops of small bowel are visible (arrows).
Lateral decubitus view of the abdomen, showing air-fluid levels consistent with intestinal obstruction (arrows).
Intussusception is a process in which a segment of intestine invaginates into the adjoining intestinal lumen, causing a bowel obstruction. intussuscipiens intussusceptum
Etiology • Intussusception is most commonly idiopathic and no anatomic lead point can be identified. Several viral gastrointestinal pathogens (rotavirus, reovirus, echovirus) may cause hypertrophy of the Peyer’s patches of the terminal ileum which may potentiate bowel intussusception. • A recognizable, anatomic lesion acting as a lead point is only found in 2-12% of all pediatric cases. The most commonly encountered anatomic lead point is a Meckel’s diverticulum. Other anatomic lead points include polyps, ectopic pancreatic or gastric rests, lymphoma, lymphosarcoma, enterogenic cyst, hamartomas (i.e., Peutz-Jeghers syndrome), submucosal hematomas (i.e., Henoch-Schonlein purpura), inverted appendiceal stumps, and anastomotic suture lines. Children with cystic fibrosis are at increased risk of intussusception possibly due to thickened inspissated stool. • Postoperative intussusception accounts for 1.5-6% of all pediatric cases of intussusception.
Clinical Presentation 1. vomiting (85%)-initially, vomiting is nonbilious and reflexive, but when the intestinal obstruction occurs, vomiting becomes bilious. 2. abdominal pain (83%)-pain is colicky, severe, and intermittent. 3. passage of blood or bloody mucous per rectum (53%). 4. a palpable abdominal mass 5. lethargy. 6. diarrhea. The classic triad of pain, vomiting, and bloody mucous stools(“red current jelly”) is present in only one third of infants with intussusception. Diarrhea may be present in 10-20% of patients.
Differential diagnosis • includes intestinal colic. • gastroenteritis. • acute appendicitis. • incarcerated hernia. • internal hernia. • volvulus.
X-ray examination • Pneumoirigograhy
Air enema showing the intussusception is in thesplenic flexure (arrow).
CT scan reveals the classic ying-yang sign of an intussusceptum inside an intussuscipiens.
Abdominal sonograph reveals the classic target sign of an intussusceptum inside an intussuscipiens.
Intussusception. (A) Longitudinal sonogram of a child with the typical clinical presentation of intussusception. This is a longitudinal sonogram through the intussusception. There are multiple lymph nodes (arrows) in the intussusception. (B) Transverse sonogram of the intussusception showing the multiple lymph nodes (arrows) within the intussusception. If lymph nodes are seen within an intussusceptum it has been reported that it is more difficult to reduce the intussusception.
(C) Transverse sonogram of an intussusception showing the color flow within the intussusceptum. This indicates that the intussusception is still viable. When no color flow is seen on Doppler, suspicion must be raised that the intussusception is no longer viable and the risk of perforation is high.
Complications: • Intestinal hemorrhage • Necrosis and bowel perforation • Shock and sepsis
Enema Reduction • Personal comfort level is probably the best contrast selection criterion • All have similar rates of reduction (75-85%) and perforation (1-2%) • End point - free reflux into small bowel and reduction of mass • Often see edema of ileocecal valve • Main goal is to prevent unnecessary open reduction, select patients who need resection
Non-operative reduction of the intussusception Richardson balloon for pneumoirigography
Principles of barium enema reduction 1. Perform nasogastric suction: administer 4 fluids or blood and antibiotics 2. Insert ungreased Foley catheter in rectum, distend ballon and pull down against levator. Strap in place 3. Wrap legs 4. Let barium run from height of 30 cm in above table 5. X-ray intermittently 6. Stop if barium column is stationary and its unchanging for 10 min 7. Reduction
Surgical treatment indication is: • a shocked child with signs of peritonism • or in whom intussusception does not resolve with a nonoperativ procedure
Operative technique: • The intussusception is milked back by progressive compression of the bowel In severe cases: • Intestinal resection • Placement of ileotransversal anastomosis • Ileostoma and caecostoma placement
BIBLIOGRAPHY • Abasiyanik A, Dasci Z, Yosunkaya A, et al: Laparoscopic-assisted pneumatic reduction of intussusception. J Pediatr Surg 1997 Aug; 32(8): 1147-8[Medline]. • Barr LL: Sonography in the infant with acute abdominal symptoms. Semin Ultrasound CT MR 1994 Aug; 15(4): 275-89[Medline]. • Boehm R, Till H: Recurrent intussusceptions in an infant that were terminated by laparoscopic ileocolonic pexie. Surg Endosc 2003 May; 17(5): 831-2[Medline]. • Chang HG, Smith PF, Ackelsberg J, et al: Intussusception, rotavirus diarrhea, and rotavirus vaccine use among children in New York State. Pediatrics 2001 Jul; 108(1): 54-60[Medline]. • Collins DL, Pinckney LE, Miller KE, et al: Hydrostatic reduction of ileocolic intussusception: a second attempt in the operating room with general anesthesia. J Pediatr 1989 Aug; 115(2): 204-7[Medline]. • Cull DL, Rosario V, Lally KP, et al: Surgical implications of Henoch-Schonlein purpura. J Pediatr Surg 1990 Jul; 25(7): 741-3[Medline]. • Dennison WM, Shaker M: Intussusception in infancy and childhood. Br J Surg 1970 Sep; 57(9): 679-84[Medline]. • DiFiore JW: Intussusception. Semin Pediatr Surg 1999 Nov; 8(4): 214-20[Medline]. • Doody DP: Intussusception. In: Oldham KT, Colombani PM, Foglia RP, eds. Surgery of Infants and Children: Scientific Principles and Practice. Lippincott-Raven; 1997: 1241-8. • Ein SH, Stephens CA: Intussusception: 354 cases in 10 years. J Pediatr Surg 1971 Feb; 6(1): 16-27[Medline]. • Eklof OA, Johanson L, Lohr G: Childhood intussusception: hydrostatic reducibility and incidence of leading points in different age groups. Pediatr Radiol 1980 Nov; 10(2): 83-6[Medline].