Download
1 / 1
10 likes | 157 Views
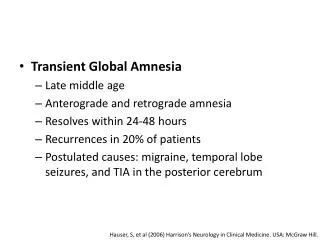
q (cue size). μ 1. recall. Store 1: hippocampus. l. l (learning). a1 (forgetting). a1. μ 2 (consolidation). μ 2. Store 2: neocortex. a1. l. a. b. c. d.

E N D
q (cue size) μ1 recall Store 1: hippocampus l l(learning) a1(forgetting) a1 μ2 (consolidation) μ2 Store 2: neocortex a1 l a. b. c. d. Fitting a Patient’s Remote Memory: Tests, Models, and Outcomesm@ meeter.nlM. Meeter11 Dept. of Psychology, Univ. of Amsterdamjaap@murre.com J.M.J. Murre1,22 Dept. of Computer Science, Univ. of Maastrichtsjanssen@fmg.uva.nl S.M.J. Janssen1The Netherlands • Selecting questions • Control data is fitted with the 2-store Memory Chain Model (MCM) of learning, amnesia and forgetting (Chessa & Murre, 2002; see fig. 4). Forgetting parameters are fitted, as well as question difficulty coefficients. This allows us to select the easiest questions for inclusion in the retrograde amnesia test. Questions are selected in such way that average difficulty is equal for different periods in the test (table 1). • Fitting patients • Individual patients answer 30-50 questions from the last six months.Their scores on these items can be fitted by three MCM variants (fig. 4). • The ‘normal’ model: just a knowledge parameter is fitted to the data • The ‘fast forgetter’ model: forgetting parameter a1 is allowed to vary. This model implies better memory for recent news than for older news • The ‘retrograde amnesia’ model with added hippocampal lesion parameter. This model implies better memory for old, consolidated news than for recent, putatively hippocampally stored news. • Assumptions • The MCM is a valid model of retention • All normal subject differences are captured by a knowledge parameter • All item differences are captured by the difficulty coefficient • Item- and subject differences interact in a multiplicative way • Parameters can be stably estimated from control data. • Results: sensitivity and specificity • In a Monte Carlo study, we simulated performance of 100 normal pseudosubjects, 100 fast forgetters and 100 patients with retrograde amnesia. These were then categorized via the fitting procedure. In a pilot test, 36 normal controls were categorized as either normal, fast forgetter or suffering from r.a. • With a strict criterion (diagnosis only made if normal model rejected with a=.05), most simulated normal controls were categorized correctly but sensitivity was mediocre (table 2). • With a less strict criterion (diagnosis made if the Akaike Information Coefficient is higher for an abnormal model than for the normal model) specificity was still good, and sensitivity was satisfactory. • Specificity was less good but still satisfactory when tested in real controls. This is not surprising: real subjects do not always follow the news with equal intensity (e.g., vacations), which will distort temporal patterns in their data. • Conclusions • The DNMT-ra allows for the first time the measurement of retrograde amnesia for short periods (e.g., months). • With help of the MCM, models incorporating hypotheses about a patient’s memory can be tested against the patient’s data. • Many issues still need to be resolved, and the real test for the DNMT-ra (i.e. diagnosing patients) is still forthcoming • Chessa, A.G. & Murre, J.M.J. (2002). A model of learning and forgetting I: The forgetting curve. Amsterdam: NeuroMod Technical Report 02-01. • Most tests of retrograde amnesia measure time in decades. We designed a test for amnesia with a resolution of months: the Daily News Memory Test-retrograde amnesia (DNMT-ra). The DNMT-ra is constructed via a script made feasible via internet. First, normal controls answer random samples of questions about the news via an Internet test. Data generated in this way is then fitted with a mathematical model of retention (the Memory Chain Model, or MCM), allowing appropriate questions to be selected from our database and to be assembled in a test by an automated script. • To diagnose a single participant with the resulting DNMT-ra, variants of the MCM are fitted to that participant’s data. These variants incorporate specific assumptions about the deficit a participant may have, allowing these hypotheses to be tested against one-another. To investigate the sensitivity and specificity of this procedure, we performed Monte Carlo simulations and did a pilot study with normal controls. Results suggested an adequate specificity and sensitivity. • Measuring retrograde amnesia • Because patients with retrograde amnesia (fig. 1) typically present after the onset of amnesia, retrograde amnesia can only be measured indirectly by comparing the memory of the patient with what is normal. Items in retrograde amnesia tests must pertain to memories that everyone has, and can be pinpointed to a date. • Kinds of tests: • Public events: questions about news events or famous faces that have to be named. • Autobiographical memory: questions about life events. • Vocabulary: neologisms that have to be defined. • Time scale of retrograde amnesia • In existing tests, the unit of time is usually a decade. This is not suitable for all forms of retrograde amnesia, which may have as duration: • Encephalitis: whole life. • Alzheimer & Korsakoff: decades • ECT & MTL lesions: years / months • Fornix cut & Head trauma : weeks • With decades as your time unit, how do you measure RA of a few months? • Recipe for a short-term RA test • Ask questions about news in last months: • make new questions every week • let controls answer your questions every week • select easiest questions • put them in daily updateable test for news of last months. • This recipe is feasible with help of internet www.memory.uva.nl • Site (fig. 1a) online since Nov. 2000 • 18,000 subjects have logged on, given biographical information, and proceeded to answer a subset of 30 to 40 questions (fig. 1b). • more than 1100 questions formulated in open & multiple-choice format • example: With what did the American submarine USS Greenville collide on Feb. 9, 2001? (options: a Canadian fishing boat, a Mexican fishing boat, a Japanese fishing boat, an Icelandic fishing boat) Results: forgetting Normal controls have yielded database with 500,000 data points that can be used to investigate forgetting: • best predictors of participant performance: frequency of reading newspapers, gender, education, age. • forgetting is independent of several such subject variables, and of item difficulty (fig. 3). a. b. Fig.4.(a). The 2-store Memory Chain Model (MCM). Memory is conceived as consisting of several chained stores, with memories being copied from one store to the next. Within one store, several copies are present. One interpretation of the model makes the hippocampus store 1, the neocortex store 2. Consolidation of memories is then the process of copying a memory from store 1 to store 2. (b) Memories are recalled by sampling part of the memory stores. If a copy of the memory is present in the sampled region, the memory is recalled. Normal fitted: m1 (knowledge param.) Retrograde Amnesia fitted: m1, l(hipp. lesion param.) Fast Forgetters fitted: m1, a1 (forgetting param.) Fig. 1. Retrograde amnesia (RA) is a loss of memory from before the onset of amnesia. E.g., in a patient with a stroke in 2001 it would be loss of memories from before 2001 Fig. 5. Possible patterns in the score on the RA test. A generally low performance (labeled uninterpretable) is difficult to interpret, as it may also be caused by lack of attention for the news. Two patterns in performance that can be distinguished are “speeded forgetting” in which the patient loses information abnormally fast, and “retrograde amnesia”, in which recent information is preferentially lost. These two patterns are associated with variants of the MCM that can be tested against the standard model (‘normal’). Fig. 2a: the portal Fig. 2b: questions as presented on the site Table 2. Classification of pseudosubjects of the Monte Carlo study, and real participants in the pilot study. Simulated fast forgetters had an a1 of 200% to 400% of the normal value, simulated patients with retrograde amnesia (ra) had 75% to 100% damage of store 1. Test details are given in table 1. Cells give the number of pseudosubjects / pilot participants diagnosed as either normal, a fast forgetter, or a r.a. patient (columns). Bold cells contain correctly classified pseudosubjects / participants. ‘sign.’ (significance) and AIC (Akaike Information Coefficient) are the two classification criteria. Table 1. Description of test 46, created on Sept. 17, 2002. It consists of 4 periods, each of 90 days. For each period, 10 questions were chosen. The fourth column gives the number of questions available from that period. Then the mean difficulty is given of the 10 easiest (‘max. f’) and 10 most difficult (‘min. f’) from that period. The ‘chosen f’ is the difficulty of the 10 questions chosen to represent the period. With this difficulty, the proportion of items is calculated that a random internet volunteer would answer correctly. Fig. 3. (a,b) Forgetting split out for Dutch participants reading many newspapers (6 a week, gray) or few newspapers (0-3 a week, black) on open (a) and multiple choice (b) questions. (c) Forgetting on open questions split out for Dutch older adults (age+60) and Dutch younger adults (age 18-24). (d). Forgetting on the 25 easiest and on 50 medium difficulty questions in the Dutch-language test. All curves were fitted with the Memory Chain Model. Models with unequal forgetting parameters for the two participant groups (a,b,c) and two question groups (d) were rejected, implying equal forgetting (power: 10% changes were detectable).